Alexander T Phan, Ankur Bhagat, Bahareh Maknouni, Momin Masroor, Mufadda Hasan
{"title":"在非流行地区获得性免疫缺陷综合征患者的播散性组织胞浆菌病(加利福尼亚)。","authors":"Alexander T Phan, Ankur Bhagat, Bahareh Maknouni, Momin Masroor, Mufadda Hasan","doi":"10.14740/jmc4097","DOIUrl":null,"url":null,"abstract":"<p><p>Histoplasmosis is caused by infection with <i>Histoplasma capsulatum</i> (<i>H. capsulatum</i>). Progressive disseminated histoplasmosis is a more severe form of histoplasmosis and is seldom diagnosed in non-endemic regions of the world owing to the fungus's geographical distribution. In the United States (USA), <i>Histoplasma capsulatum</i> is classically known to be endemic to the Mississippi and Ohio River valleys, and cases in non-endemic areas, such as the southwest USA, are exceedingly rare. Patients with acquired immunodeficiency syndrome (AIDS) are at risk for infection with <i>H. capsulatum</i>, and failure to recognize and treat histoplasmosis may be devastating to patients. In non-endemic regions, the proposed mechanism for disseminated histoplasmosis in AIDS patients is reactivation of a previous infection. Here, we present the case of a young male patient who presented to a southern California hospital with diarrhea, was diagnosed with AIDS, and developed acute hypoxic respiratory failure. Chest imaging revealed diffuse reticulonodular opacities, and histoplasmosis was confirmed by urine and serologic examination. He was subsequently treated with liposomal amphotericin B and safely discharged from the hospital with oral itraconazole therapy. This case contributes to the current limited body of literature citing histoplasmosis infections in California, and clinicians should consider histoplasmosis as a differential diagnosis in non-endemic regions.</p>","PeriodicalId":16279,"journal":{"name":"Journal of Medical Cases","volume":"14 7","pages":"260-264"},"PeriodicalIF":0.0000,"publicationDate":"2023-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/71/ef/jmc-14-260.PMC10409541.pdf","citationCount":"0","resultStr":"{\"title\":\"Disseminated Histoplasmosis in a Patient With Acquired Immunodeficiency Syndrome in a Non-Endemic Region (California).\",\"authors\":\"Alexander T Phan, Ankur Bhagat, Bahareh Maknouni, Momin Masroor, Mufadda Hasan\",\"doi\":\"10.14740/jmc4097\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Histoplasmosis is caused by infection with <i>Histoplasma capsulatum</i> (<i>H. capsulatum</i>). Progressive disseminated histoplasmosis is a more severe form of histoplasmosis and is seldom diagnosed in non-endemic regions of the world owing to the fungus's geographical distribution. In the United States (USA), <i>Histoplasma capsulatum</i> is classically known to be endemic to the Mississippi and Ohio River valleys, and cases in non-endemic areas, such as the southwest USA, are exceedingly rare. Patients with acquired immunodeficiency syndrome (AIDS) are at risk for infection with <i>H. capsulatum</i>, and failure to recognize and treat histoplasmosis may be devastating to patients. In non-endemic regions, the proposed mechanism for disseminated histoplasmosis in AIDS patients is reactivation of a previous infection. Here, we present the case of a young male patient who presented to a southern California hospital with diarrhea, was diagnosed with AIDS, and developed acute hypoxic respiratory failure. Chest imaging revealed diffuse reticulonodular opacities, and histoplasmosis was confirmed by urine and serologic examination. He was subsequently treated with liposomal amphotericin B and safely discharged from the hospital with oral itraconazole therapy. This case contributes to the current limited body of literature citing histoplasmosis infections in California, and clinicians should consider histoplasmosis as a differential diagnosis in non-endemic regions.</p>\",\"PeriodicalId\":16279,\"journal\":{\"name\":\"Journal of Medical Cases\",\"volume\":\"14 7\",\"pages\":\"260-264\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/71/ef/jmc-14-260.PMC10409541.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Medical Cases\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14740/jmc4097\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Medical Cases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/jmc4097","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Disseminated Histoplasmosis in a Patient With Acquired Immunodeficiency Syndrome in a Non-Endemic Region (California).
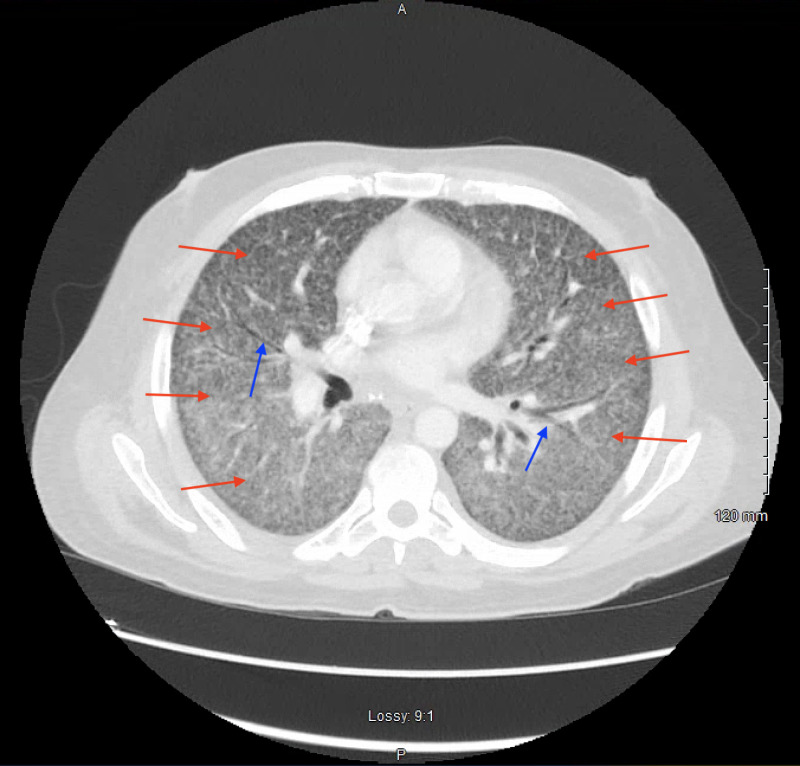
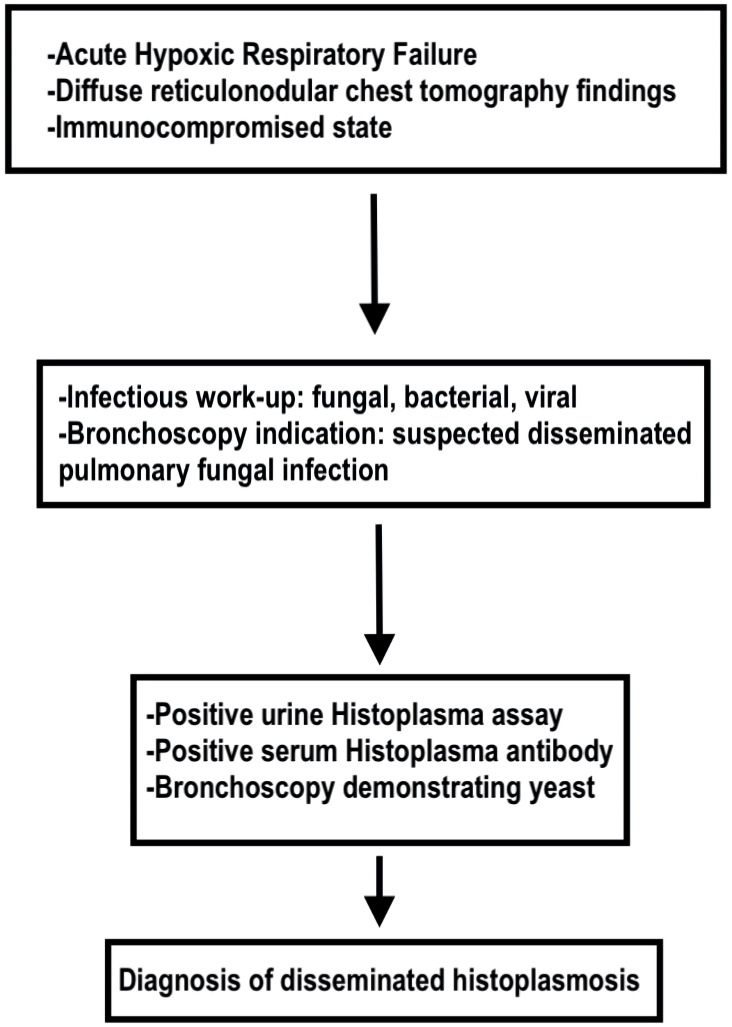
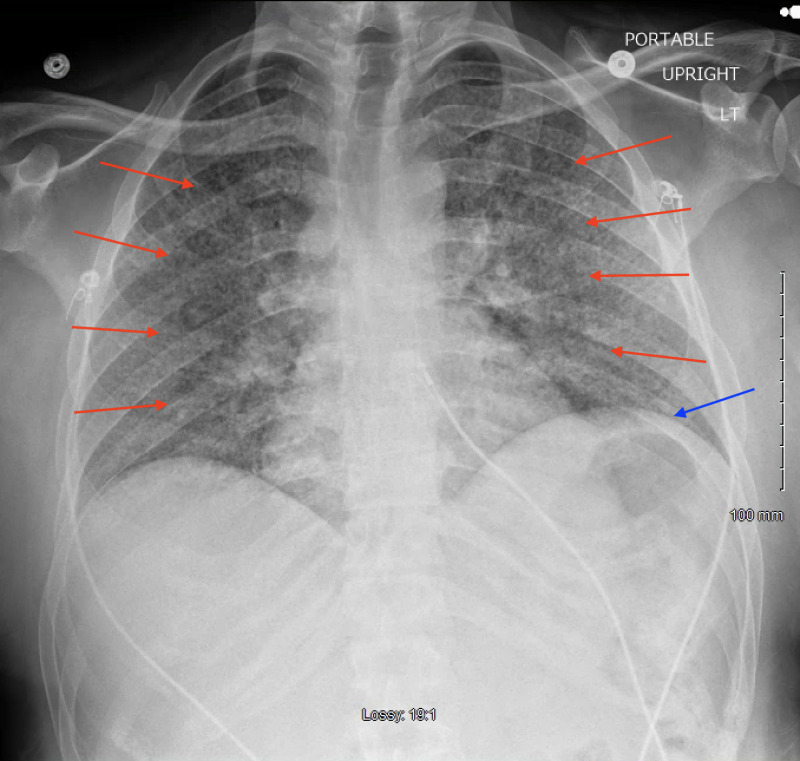
Histoplasmosis is caused by infection with Histoplasma capsulatum (H. capsulatum). Progressive disseminated histoplasmosis is a more severe form of histoplasmosis and is seldom diagnosed in non-endemic regions of the world owing to the fungus's geographical distribution. In the United States (USA), Histoplasma capsulatum is classically known to be endemic to the Mississippi and Ohio River valleys, and cases in non-endemic areas, such as the southwest USA, are exceedingly rare. Patients with acquired immunodeficiency syndrome (AIDS) are at risk for infection with H. capsulatum, and failure to recognize and treat histoplasmosis may be devastating to patients. In non-endemic regions, the proposed mechanism for disseminated histoplasmosis in AIDS patients is reactivation of a previous infection. Here, we present the case of a young male patient who presented to a southern California hospital with diarrhea, was diagnosed with AIDS, and developed acute hypoxic respiratory failure. Chest imaging revealed diffuse reticulonodular opacities, and histoplasmosis was confirmed by urine and serologic examination. He was subsequently treated with liposomal amphotericin B and safely discharged from the hospital with oral itraconazole therapy. This case contributes to the current limited body of literature citing histoplasmosis infections in California, and clinicians should consider histoplasmosis as a differential diagnosis in non-endemic regions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


