Sintra Eyre Med. Lic., Jenny Stenberg PhD, Ola Wallengren PhD, David Keane PhD, Carla M. Avesani PhD, Ingvar Bosaeus MD, PhD, Naomi Clyne MD, PhD, Olof Heimbürger MD, PhD, Ainhoa Indurain MD, Ann-Cathrine Johansson MD, PhD, Bengt Lindholm MD, PhD, Fernando Seoane, Mia Trondsen MSc, for the SWEBIS network
{"title":"慢性肾病患者的生物阻抗分析","authors":"Sintra Eyre Med. Lic., Jenny Stenberg PhD, Ola Wallengren PhD, David Keane PhD, Carla M. Avesani PhD, Ingvar Bosaeus MD, PhD, Naomi Clyne MD, PhD, Olof Heimbürger MD, PhD, Ainhoa Indurain MD, Ann-Cathrine Johansson MD, PhD, Bengt Lindholm MD, PhD, Fernando Seoane, Mia Trondsen MSc, for the SWEBIS network","doi":"10.1111/jorc.12474","DOIUrl":null,"url":null,"abstract":"<p>In recent years the use of bioimpedance analysis (BIA) for assessment of fluid status as well as body composition as a mean to assess nutritional status in CKD has increased. The interest in the method is due to the associations between fluid overload and cardiovascular disease, and between fluid overload and malnutrition, both of which contribute to an increased risk of morbidity and mortality (Hur et al., <span>2013</span>; Onofriescu et al., <span>2014</span>). Moreover, BIA devices are suitable for clinical use, since they are portable, easy to use and, with a median to low price. However, the results can be difficult to interpret and integrate into routine clinical care, and although impedance measurements can contribute to an increased understanding of the patient's fluid balance, the results should be used with caution and in combination with other physiological parameters and clinical assessments (de Ruiter et al., <span>2020</span>; Scotland et al., <span>2018</span>). The aim of this editorial is to contribute to increased awareness of the benefits and limitations of using bioimpedance in patients with CKD with or without dialysis, and contribute to improving the measurement quality, facilitating interpretations, and highlighting possible sources of error.</p><p>BIA can be defined as the resistance measured by a weak alternating current when conducted through biological tissue. The conductivity differs between different tissues, which makes it possible to estimate body composition and fluid balance. BIA equipment measures impedance, which includes the <i>reactance</i> (capacitive impedance in cell membranes and other structures) and <i>resistance</i> (resistance due to extracellular [ECW] and intracellular water [ICW]). These variables can be measured with good precision and reproducibility between different devices (Kyle et al., <span>2004</span>).</p><p>However, it is of fundamental importance to understand the limitations of BIA technology to avoid unrealistic expectations of measurement accuracy and precision (Ward, <span>2019</span>). Deriving body composition information from impedance data includes estimated and assumed parameters and the use of population-averaged factors, such as body shape. Although it is plausible that prediction equations could be improved by including more individual-level information (e.g., the use of plasma sodium to improve estimations of tissue resistivity (Mitsides et al., <span>2020</span>; Schneditz et al., <span>2023</span>) this would have huge implications for the ease of use and applicability of the technology.</p><p>Variations in agreement between different impedance techniques and devices as well as with reference methods for measuring body composition can largely be attributed to the choice of method and device-specific software (Kyle, <span>2004</span>; Kyle et al., <span>2004</span>; Sheean et al., <span>2020</span>). Also, each manufacturer of BIA equipment designs its own software for analysis and description of measurement results; this makes direct comparisons between different devices uncertain, and it would be difficult to give universal advice on how to use bioimpedance in day-to-day clinical management of patients with CKD. Therefore, although many of the guiding principles in this paper can be translatable to various devices, we will hence forward primarily be referring to the Body Composition Monitor (BCM®; Bad Homburg) a device which has been validated in patients with CKD (Davies et al., <span>2017</span>; Marcelli et al., <span>2015</span>; Wabel et al., <span>2009</span>).</p><p>As kidney failure progresses from early stages through to end-stage kidney failure, body composition is increasingly affected, including fluid retention and loss of muscle mass. Unless bioimpedance results deviate significantly from reference values, a single measurement provides limited information, but repeated measurements over time provide the most valuable information. If the measurement conditions deviate from the normal, it is especially important to have a structured and uniform methodology. Carefully conducted measurements, performed over time, probably reflect actual changes in body composition (Kyle, <span>2004</span>; Kyle et al., <span>2004</span>; van der Sande et al., <span>2020</span>). When conducting impedance measurements, pay attention to the recommendations in Table 1.</p><p>An impedance measurement generates a multitude of data. Impedance devices of various manufactures may report fluid balance and body composition output in different ways. For assessment of fluid status and nutritional status with bioimpedance, the variables in Tables 2 and 3 are commonly used:</p><p>Epidemiological studies clearly demonstrate the association between BIS measurements and important outcomes for HD patients at the population level. However, results from clinical trials suggest that the incorporation of BIS into routine clinical management is challenging. Unless results from BIS measurements deviate significantly from reference values, a single measurement provides limited information. Carefully conducted measurements, however, performed over time, probably reflect actual changes in fluid status and body composition. If the measurement conditions deviate from the normal, it is especially important to have a structured and uniform methodology for follow up and, if possible, perform repeated measurements or use a reference method, for example, dual-energy X-ray absorptiometry. We believe that by better understanding of the fundamental differences between bioimpedance devices, principles of measurement and incorporation of the results with clinical assessment as part of decision support tools may better support use of BIS at the individual level.</p><p>The members of the SWEBIS network agree to the submission of the manuscript to the Journal of Renal Care. All authors fulfil the ICMJE requirements for authorship and contributed to the manuscript. Sintra Eyre and Jenny Stenberg were principal project leaders and responsible for the main drafting of the manuscript, with special contributions, design and coordination made by Ola Wallengren and David Keane. All the other authors (Carla M. Avesani, Ingvar Bosaeus, Naomi Clyne, Olof Heimbürger, Ainhoa Indurain, Ann-Cathrine Johansson, Bengt Lindholm, Fernando Seoane, Mia Trondsen) made critical revisions and participated with important intellectual content, read, and approved the final manuscript.</p><p>Jenny Stenberg: Honoraria for lectures from AstraZeneca, Baxter Healthcare and Fresenius Medical Care. Ola Wallengren: Personal speakers fee from Fresenius Kabi AB for educational lectures. Carla M. Avesani: C. M. A. declares no conflict of interest with the current paper. C. M. A. received payment for lectures from Astra Zeneca, Fresenius Medical Care and Baxter healthcare and participation in Advisory board for Astra Zeneca. Olof Heimbürger: Honoraria for lectures from Baxter Healthcare, Fresenius Medical Care, Astra Zeneca, ewimed and Vifor. Ann-Cathrine Johansson: Personal speakers fee from Fresenius AB. Bengt Lindholm: Affiliated with Baxter Healthcare: Previous employment; owns stock; Baxter Novum is supported by grant from Baxter Healthcare to Karolinska Institutet. The remaining authors declare no conflict of interest.</p><p>This guideline for the clinical use of bioimpedance in patients with CKD was developed by the Swedish Bioimpedance Network (SWEBIS), which is an interprofessional network of people interested in the clinical application of bioimpedance in patients with chronic kidney disease (CKD). The network, which was initiated in 2014, consists of dieticians (SE, CA, OW), physiotherapists (MT), nurses (JS), physicians (ACJ, IB, NC, OH, AI, BL), and engineers/physicist (DK, FS).</p>","PeriodicalId":16947,"journal":{"name":"Journal of renal care","volume":"49 3","pages":"147-157"},"PeriodicalIF":1.5000,"publicationDate":"2023-07-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jorc.12474","citationCount":"0","resultStr":"{\"title\":\"Bioimpedance analysis in patients with chronic kidney disease\",\"authors\":\"Sintra Eyre Med. Lic., Jenny Stenberg PhD, Ola Wallengren PhD, David Keane PhD, Carla M. Avesani PhD, Ingvar Bosaeus MD, PhD, Naomi Clyne MD, PhD, Olof Heimbürger MD, PhD, Ainhoa Indurain MD, Ann-Cathrine Johansson MD, PhD, Bengt Lindholm MD, PhD, Fernando Seoane, Mia Trondsen MSc, for the SWEBIS network\",\"doi\":\"10.1111/jorc.12474\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>In recent years the use of bioimpedance analysis (BIA) for assessment of fluid status as well as body composition as a mean to assess nutritional status in CKD has increased. The interest in the method is due to the associations between fluid overload and cardiovascular disease, and between fluid overload and malnutrition, both of which contribute to an increased risk of morbidity and mortality (Hur et al., <span>2013</span>; Onofriescu et al., <span>2014</span>). Moreover, BIA devices are suitable for clinical use, since they are portable, easy to use and, with a median to low price. However, the results can be difficult to interpret and integrate into routine clinical care, and although impedance measurements can contribute to an increased understanding of the patient's fluid balance, the results should be used with caution and in combination with other physiological parameters and clinical assessments (de Ruiter et al., <span>2020</span>; Scotland et al., <span>2018</span>). The aim of this editorial is to contribute to increased awareness of the benefits and limitations of using bioimpedance in patients with CKD with or without dialysis, and contribute to improving the measurement quality, facilitating interpretations, and highlighting possible sources of error.</p><p>BIA can be defined as the resistance measured by a weak alternating current when conducted through biological tissue. The conductivity differs between different tissues, which makes it possible to estimate body composition and fluid balance. BIA equipment measures impedance, which includes the <i>reactance</i> (capacitive impedance in cell membranes and other structures) and <i>resistance</i> (resistance due to extracellular [ECW] and intracellular water [ICW]). These variables can be measured with good precision and reproducibility between different devices (Kyle et al., <span>2004</span>).</p><p>However, it is of fundamental importance to understand the limitations of BIA technology to avoid unrealistic expectations of measurement accuracy and precision (Ward, <span>2019</span>). Deriving body composition information from impedance data includes estimated and assumed parameters and the use of population-averaged factors, such as body shape. Although it is plausible that prediction equations could be improved by including more individual-level information (e.g., the use of plasma sodium to improve estimations of tissue resistivity (Mitsides et al., <span>2020</span>; Schneditz et al., <span>2023</span>) this would have huge implications for the ease of use and applicability of the technology.</p><p>Variations in agreement between different impedance techniques and devices as well as with reference methods for measuring body composition can largely be attributed to the choice of method and device-specific software (Kyle, <span>2004</span>; Kyle et al., <span>2004</span>; Sheean et al., <span>2020</span>). Also, each manufacturer of BIA equipment designs its own software for analysis and description of measurement results; this makes direct comparisons between different devices uncertain, and it would be difficult to give universal advice on how to use bioimpedance in day-to-day clinical management of patients with CKD. Therefore, although many of the guiding principles in this paper can be translatable to various devices, we will hence forward primarily be referring to the Body Composition Monitor (BCM®; Bad Homburg) a device which has been validated in patients with CKD (Davies et al., <span>2017</span>; Marcelli et al., <span>2015</span>; Wabel et al., <span>2009</span>).</p><p>As kidney failure progresses from early stages through to end-stage kidney failure, body composition is increasingly affected, including fluid retention and loss of muscle mass. Unless bioimpedance results deviate significantly from reference values, a single measurement provides limited information, but repeated measurements over time provide the most valuable information. If the measurement conditions deviate from the normal, it is especially important to have a structured and uniform methodology. Carefully conducted measurements, performed over time, probably reflect actual changes in body composition (Kyle, <span>2004</span>; Kyle et al., <span>2004</span>; van der Sande et al., <span>2020</span>). When conducting impedance measurements, pay attention to the recommendations in Table 1.</p><p>An impedance measurement generates a multitude of data. Impedance devices of various manufactures may report fluid balance and body composition output in different ways. For assessment of fluid status and nutritional status with bioimpedance, the variables in Tables 2 and 3 are commonly used:</p><p>Epidemiological studies clearly demonstrate the association between BIS measurements and important outcomes for HD patients at the population level. However, results from clinical trials suggest that the incorporation of BIS into routine clinical management is challenging. Unless results from BIS measurements deviate significantly from reference values, a single measurement provides limited information. Carefully conducted measurements, however, performed over time, probably reflect actual changes in fluid status and body composition. If the measurement conditions deviate from the normal, it is especially important to have a structured and uniform methodology for follow up and, if possible, perform repeated measurements or use a reference method, for example, dual-energy X-ray absorptiometry. We believe that by better understanding of the fundamental differences between bioimpedance devices, principles of measurement and incorporation of the results with clinical assessment as part of decision support tools may better support use of BIS at the individual level.</p><p>The members of the SWEBIS network agree to the submission of the manuscript to the Journal of Renal Care. All authors fulfil the ICMJE requirements for authorship and contributed to the manuscript. Sintra Eyre and Jenny Stenberg were principal project leaders and responsible for the main drafting of the manuscript, with special contributions, design and coordination made by Ola Wallengren and David Keane. All the other authors (Carla M. Avesani, Ingvar Bosaeus, Naomi Clyne, Olof Heimbürger, Ainhoa Indurain, Ann-Cathrine Johansson, Bengt Lindholm, Fernando Seoane, Mia Trondsen) made critical revisions and participated with important intellectual content, read, and approved the final manuscript.</p><p>Jenny Stenberg: Honoraria for lectures from AstraZeneca, Baxter Healthcare and Fresenius Medical Care. Ola Wallengren: Personal speakers fee from Fresenius Kabi AB for educational lectures. Carla M. Avesani: C. M. A. declares no conflict of interest with the current paper. C. M. A. received payment for lectures from Astra Zeneca, Fresenius Medical Care and Baxter healthcare and participation in Advisory board for Astra Zeneca. Olof Heimbürger: Honoraria for lectures from Baxter Healthcare, Fresenius Medical Care, Astra Zeneca, ewimed and Vifor. Ann-Cathrine Johansson: Personal speakers fee from Fresenius AB. Bengt Lindholm: Affiliated with Baxter Healthcare: Previous employment; owns stock; Baxter Novum is supported by grant from Baxter Healthcare to Karolinska Institutet. The remaining authors declare no conflict of interest.</p><p>This guideline for the clinical use of bioimpedance in patients with CKD was developed by the Swedish Bioimpedance Network (SWEBIS), which is an interprofessional network of people interested in the clinical application of bioimpedance in patients with chronic kidney disease (CKD). The network, which was initiated in 2014, consists of dieticians (SE, CA, OW), physiotherapists (MT), nurses (JS), physicians (ACJ, IB, NC, OH, AI, BL), and engineers/physicist (DK, FS).</p>\",\"PeriodicalId\":16947,\"journal\":{\"name\":\"Journal of renal care\",\"volume\":\"49 3\",\"pages\":\"147-157\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2023-07-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/jorc.12474\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of renal care\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/jorc.12474\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"NURSING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of renal care","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/jorc.12474","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"NURSING","Score":null,"Total":0}
引用次数: 0
摘要
近年来,使用生物阻抗分析(BIA)来评估液体状态和身体成分,作为评估慢性肾病营养状况的一种手段已经增加。之所以对该方法感兴趣,是因为液体过量与心血管疾病之间以及液体过量与营养不良之间存在关联,这两者都导致发病率和死亡率风险增加(Hur等人,2013年;Onofriescu et al., 2014)。此外,BIA装置适合临床使用,因为它们便携,易于使用,价格中位数到较低。然而,结果可能难以解释并融入常规临床护理,尽管阻抗测量有助于增加对患者液体平衡的了解,但应谨慎使用结果,并与其他生理参数和临床评估相结合(de Ruiter et al., 2020;苏格兰等人,2018)。这篇社论的目的是提高人们对在CKD伴透析或不伴透析患者中使用生物阻抗的益处和局限性的认识,并有助于提高测量质量,促进解释,并强调可能的误差来源。BIA可以定义为弱交流电通过生物组织时测量的电阻。不同组织之间的电导率不同,这使得估计身体成分和液体平衡成为可能。BIA设备测量阻抗,包括电抗(细胞膜和其他结构中的电容阻抗)和电阻(由于细胞外[ECW]和细胞内水[ICW]引起的电阻)。这些变量可以在不同的设备之间以良好的精度和再现性进行测量(Kyle et al., 2004)。然而,了解BIA技术的局限性是至关重要的,以避免对测量精度和精度的不切实际的期望(Ward, 2019)。从阻抗数据中获得身体成分信息包括估计的和假设的参数,以及使用人口平均因素,如体型。尽管通过包含更多个人层面的信息(例如,使用血浆钠来改进组织电阻率的估计),预测方程可能会得到改进(Mitsides等人,2020;Schneditz et al., 2023)这将对该技术的易用性和适用性产生巨大影响。不同阻抗技术和设备之间的一致性差异以及测量身体成分的参考方法在很大程度上可归因于方法和设备特定软件的选择(Kyle, 2004;Kyle et al., 2004;Sheean et al., 2020)。此外,每个BIA设备制造商都设计了自己的软件来分析和描述测量结果;这使得不同设备之间的直接比较不确定,并且很难给出关于如何在CKD患者的日常临床管理中使用生物阻抗的普遍建议。因此,尽管本文中的许多指导原则可以翻译为各种设备,但我们将主要参考身体成分监测器(BCM®;Bad Homburg)一种已在CKD患者中得到验证的设备(Davies等人,2017;Marcelli et al., 2015;Wabel et al., 2009)。随着肾衰竭从早期发展到终末期,身体成分受到越来越大的影响,包括液体潴留和肌肉量的减少。除非生物阻抗结果明显偏离参考值,否则单次测量提供的信息有限,但随着时间的推移重复测量提供最有价值的信息。如果测量条件偏离正常,有一个结构化和统一的方法是特别重要的。仔细进行的测量,随着时间的推移,可能反映出身体成分的实际变化(Kyle, 2004;Kyle et al., 2004;van der Sande et al., 2020)。在进行阻抗测量时,请注意表1中的建议。阻抗测量产生大量的数据。不同制造商的阻抗装置可能以不同的方式报告流体平衡和身体成分输出。对于用生物阻抗评估体液状态和营养状况,表2和表3中的变量是常用的:流行病学研究清楚地表明,在人群水平上,BIS测量与HD患者的重要结果之间存在关联。然而,临床试验结果表明,将BIS纳入常规临床管理是具有挑战性的。除非BIS测量结果明显偏离参考值,否则单次测量提供的信息有限。然而,随着时间的推移,仔细进行的测量可能反映出体液状态和身体成分的实际变化。 如果测量条件偏离正常,特别重要的是要有一个结构化和统一的跟踪方法,如果可能的话,进行重复测量或使用参考方法,例如双能x射线吸收测定法。我们认为,通过更好地理解生物阻抗装置之间的基本差异,测量原理以及将结果与临床评估结合起来作为决策支持工具的一部分,可以更好地支持在个人层面使用BIS。SWEBIS网络的成员同意将稿件提交给《肾脏护理杂志》。所有作者都符合ICMJE对作者身份的要求,并对稿件做出了贡献。Sintra Eyre和Jenny Stenberg是主要的项目负责人,负责手稿的主要起草,Ola Wallengren和David Keane做出了特殊的贡献、设计和协调。所有其他作者(Carla M. Avesani, Ingvar Bosaeus, Naomi Clyne, Olof heimb<e:1> rger, Ainhoa Indurain, ann - catherine Johansson, Bengt Lindholm, Fernando Seoane, Mia Trondsen)都进行了重要的修改,并参与了重要的知识内容,阅读并批准了最终的手稿。Jenny Stenberg:感谢阿斯利康,百特医疗和费森尤斯医疗的讲座。奥拉·瓦伦格伦:费森尤斯·卡比公司的个人演讲费,用于教育讲座。Carla M. Avesani: c.m.a.声明与当前论文没有利益冲突。c.m.a.收到来自Astra Zeneca、Fresenius Medical Care和Baxter healthcare的讲座报酬,并参加Astra Zeneca的顾问委员会。Olof heimbrger:感谢百特医疗、费森尤斯医疗、阿斯利康、ewimed和Vifor的讲座。安-凯瑟琳·约翰逊:费森尤斯公司个人演讲费本特·林德霍尔姆:隶属于百特医疗保健公司:以前的工作;拥有股票;百特Novum由百特医疗保健公司向卡罗林斯卡医学院提供资助。其余作者声明没有利益冲突。该指南是由瑞典生物阻抗网络(SWEBIS)制定的,该网络是一个对生物阻抗在慢性肾脏疾病(CKD)患者临床应用感兴趣的跨专业网络。该网络于2014年启动,由营养师(SE, CA, OW),物理治疗师(MT),护士(JS),医生(ACJ, IB, NC, OH, AI, BL)和工程师/物理学家(DK, FS)组成。
Bioimpedance analysis in patients with chronic kidney disease
In recent years the use of bioimpedance analysis (BIA) for assessment of fluid status as well as body composition as a mean to assess nutritional status in CKD has increased. The interest in the method is due to the associations between fluid overload and cardiovascular disease, and between fluid overload and malnutrition, both of which contribute to an increased risk of morbidity and mortality (Hur et al., 2013; Onofriescu et al., 2014). Moreover, BIA devices are suitable for clinical use, since they are portable, easy to use and, with a median to low price. However, the results can be difficult to interpret and integrate into routine clinical care, and although impedance measurements can contribute to an increased understanding of the patient's fluid balance, the results should be used with caution and in combination with other physiological parameters and clinical assessments (de Ruiter et al., 2020; Scotland et al., 2018). The aim of this editorial is to contribute to increased awareness of the benefits and limitations of using bioimpedance in patients with CKD with or without dialysis, and contribute to improving the measurement quality, facilitating interpretations, and highlighting possible sources of error.
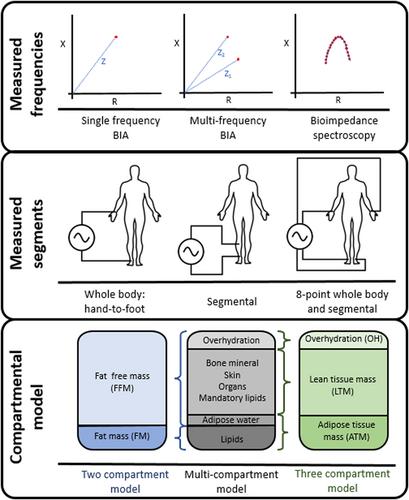
BIA can be defined as the resistance measured by a weak alternating current when conducted through biological tissue. The conductivity differs between different tissues, which makes it possible to estimate body composition and fluid balance. BIA equipment measures impedance, which includes the reactance (capacitive impedance in cell membranes and other structures) and resistance (resistance due to extracellular [ECW] and intracellular water [ICW]). These variables can be measured with good precision and reproducibility between different devices (Kyle et al., 2004).
However, it is of fundamental importance to understand the limitations of BIA technology to avoid unrealistic expectations of measurement accuracy and precision (Ward, 2019). Deriving body composition information from impedance data includes estimated and assumed parameters and the use of population-averaged factors, such as body shape. Although it is plausible that prediction equations could be improved by including more individual-level information (e.g., the use of plasma sodium to improve estimations of tissue resistivity (Mitsides et al., 2020; Schneditz et al., 2023) this would have huge implications for the ease of use and applicability of the technology.
Variations in agreement between different impedance techniques and devices as well as with reference methods for measuring body composition can largely be attributed to the choice of method and device-specific software (Kyle, 2004; Kyle et al., 2004; Sheean et al., 2020). Also, each manufacturer of BIA equipment designs its own software for analysis and description of measurement results; this makes direct comparisons between different devices uncertain, and it would be difficult to give universal advice on how to use bioimpedance in day-to-day clinical management of patients with CKD. Therefore, although many of the guiding principles in this paper can be translatable to various devices, we will hence forward primarily be referring to the Body Composition Monitor (BCM®; Bad Homburg) a device which has been validated in patients with CKD (Davies et al., 2017; Marcelli et al., 2015; Wabel et al., 2009).
As kidney failure progresses from early stages through to end-stage kidney failure, body composition is increasingly affected, including fluid retention and loss of muscle mass. Unless bioimpedance results deviate significantly from reference values, a single measurement provides limited information, but repeated measurements over time provide the most valuable information. If the measurement conditions deviate from the normal, it is especially important to have a structured and uniform methodology. Carefully conducted measurements, performed over time, probably reflect actual changes in body composition (Kyle, 2004; Kyle et al., 2004; van der Sande et al., 2020). When conducting impedance measurements, pay attention to the recommendations in Table 1.
An impedance measurement generates a multitude of data. Impedance devices of various manufactures may report fluid balance and body composition output in different ways. For assessment of fluid status and nutritional status with bioimpedance, the variables in Tables 2 and 3 are commonly used:
Epidemiological studies clearly demonstrate the association between BIS measurements and important outcomes for HD patients at the population level. However, results from clinical trials suggest that the incorporation of BIS into routine clinical management is challenging. Unless results from BIS measurements deviate significantly from reference values, a single measurement provides limited information. Carefully conducted measurements, however, performed over time, probably reflect actual changes in fluid status and body composition. If the measurement conditions deviate from the normal, it is especially important to have a structured and uniform methodology for follow up and, if possible, perform repeated measurements or use a reference method, for example, dual-energy X-ray absorptiometry. We believe that by better understanding of the fundamental differences between bioimpedance devices, principles of measurement and incorporation of the results with clinical assessment as part of decision support tools may better support use of BIS at the individual level.
The members of the SWEBIS network agree to the submission of the manuscript to the Journal of Renal Care. All authors fulfil the ICMJE requirements for authorship and contributed to the manuscript. Sintra Eyre and Jenny Stenberg were principal project leaders and responsible for the main drafting of the manuscript, with special contributions, design and coordination made by Ola Wallengren and David Keane. All the other authors (Carla M. Avesani, Ingvar Bosaeus, Naomi Clyne, Olof Heimbürger, Ainhoa Indurain, Ann-Cathrine Johansson, Bengt Lindholm, Fernando Seoane, Mia Trondsen) made critical revisions and participated with important intellectual content, read, and approved the final manuscript.
Jenny Stenberg: Honoraria for lectures from AstraZeneca, Baxter Healthcare and Fresenius Medical Care. Ola Wallengren: Personal speakers fee from Fresenius Kabi AB for educational lectures. Carla M. Avesani: C. M. A. declares no conflict of interest with the current paper. C. M. A. received payment for lectures from Astra Zeneca, Fresenius Medical Care and Baxter healthcare and participation in Advisory board for Astra Zeneca. Olof Heimbürger: Honoraria for lectures from Baxter Healthcare, Fresenius Medical Care, Astra Zeneca, ewimed and Vifor. Ann-Cathrine Johansson: Personal speakers fee from Fresenius AB. Bengt Lindholm: Affiliated with Baxter Healthcare: Previous employment; owns stock; Baxter Novum is supported by grant from Baxter Healthcare to Karolinska Institutet. The remaining authors declare no conflict of interest.
This guideline for the clinical use of bioimpedance in patients with CKD was developed by the Swedish Bioimpedance Network (SWEBIS), which is an interprofessional network of people interested in the clinical application of bioimpedance in patients with chronic kidney disease (CKD). The network, which was initiated in 2014, consists of dieticians (SE, CA, OW), physiotherapists (MT), nurses (JS), physicians (ACJ, IB, NC, OH, AI, BL), and engineers/physicist (DK, FS).
期刊介绍:
The Journal of Renal Care (JORC), formally EDTNA/ERCA Journal, is the official publication of the European Dialysis and Transplant Nursing Association/European Renal Care Association (EDTNA/ERCA).
The Journal of Renal Care is an international peer-reviewed journal for the multi-professional health care team caring for people with kidney disease and those who research this specialised area of health care. Kidney disease is a chronic illness with four basic treatments: haemodialysis, peritoneal dialysis conservative management and transplantation, which includes emptive transplantation, living donor & cadavaric transplantation. The continuous world-wide increase of people with chronic kidney disease (CKD) means that research and shared knowledge into the causes and treatment is vital to delay the progression of CKD and to improve treatments and the care given.
The Journal of Renal Care is an important journal for all health-care professionals working in this and associated conditions, such as diabetes and cardio-vascular disease amongst others. It covers the trajectory of the disease from the first diagnosis to palliative care and includes acute renal injury. The Journal of Renal Care accepts that kidney disease affects not only the patients but also their families and significant others and provides a forum for both the psycho-social and physiological aspects of the disease.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


