Yván R Persia-Paulino, Javier Cuevas-Pérez, Rodrigo Fernández-Asensio, Alejandro Junco-Vicente, Lisardo Iglesias-Fraile, Ana Ayesta
{"title":"恶性冠状血管痉挛难治性硝酸盐:使用克利夫地平作为紧急冠状血管扩张剂。","authors":"Yván R Persia-Paulino, Javier Cuevas-Pérez, Rodrigo Fernández-Asensio, Alejandro Junco-Vicente, Lisardo Iglesias-Fraile, Ana Ayesta","doi":"10.24875/ACM.21000251","DOIUrl":null,"url":null,"abstract":"Coronary artery vasospasm is a cause of chest pain described more than 50 years ago by Prinzmetal et al., named as variant angina1. Now, it is commonly known as Prinzmetal angina or vasospastic angina (VA). Patients with VA have episodes of oppressive chest pain, characterized by diurnal variation and not with exercise (even at rest), that have good response to short acting oral nitrates and oral calcium channel blockers (CCB)1. Some patients with VA develop malignant ventricular arrythmias during ischemic episodes that lead to sudden death2. Although VA usually has a good response to oral nitrates and oral CCB, treatment of patients that cannot tolerate oral drugs (on the acute phase of sudden death, hemodynamically unstable or patients on mechanical ventilation) options are very reduced. In this case report, we present a patient with an outpatient aborted sudden death due to VA with frequent episodes of coronary arteries vasospasms with malignant ventricular arrythmias refractory to intravenous nitrates that responded to clevidipine, an intravenous CCB. A 65-years-old male patient was brought to the emergency room due to out-of-hospital cardiac arrest. Past medical history of hypertriglyceridemia and was an active smoker. Chronic medication included atorvastatin 20 mg once daily (OD) and acetylsalicylic acid 100 mg (OD). The patient suffered cardiac arrest while traveling on public bus and basic life support maneuvers were started until medical assistance arrived. The automated external defibrillator showed a ventricular fibrillation (VF) and after 2 shocks of 200 Joules (J) and 15 min of cardiopulmonary resuscitation maneuvers the patient recovered pulse. The 12-lead electrocardiogram (ECG) showed sinus tachycardia without signs of myocardial ischemia. The patient was transferred to the hospital with mechanical ventilation support. Once on the emergency room, the patient was hemodynamically stable without vasoactive drugs. No remarkable findings on physical examination. The ECG showed a sinus tachycardia without alterations suggestive of myocardial ischemia (Fig. 1A). An emergency echocardiogram was performed and normal size non-hypertrophic left ventricle with mild global hypokinesia (no regional alterations in contraction suggestive of coronary artery disease) was found. Anyways, hemodynamics laboratory was contacted for an urgent coronarography to exclude myocardial ischemia as the cause of VF.","PeriodicalId":8360,"journal":{"name":"Archivos de cardiologia de Mexico","volume":"92 4","pages":"537-540"},"PeriodicalIF":0.7000,"publicationDate":"2022-10-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/97/aa/6936AX214-ACM-92-537.PMC9681519.pdf","citationCount":"0","resultStr":"{\"title\":\"Malignant coronary vasospasm refractory to nitrates: Using clevidipine as an emergent coronary vasodilator.\",\"authors\":\"Yván R Persia-Paulino, Javier Cuevas-Pérez, Rodrigo Fernández-Asensio, Alejandro Junco-Vicente, Lisardo Iglesias-Fraile, Ana Ayesta\",\"doi\":\"10.24875/ACM.21000251\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"Coronary artery vasospasm is a cause of chest pain described more than 50 years ago by Prinzmetal et al., named as variant angina1. Now, it is commonly known as Prinzmetal angina or vasospastic angina (VA). Patients with VA have episodes of oppressive chest pain, characterized by diurnal variation and not with exercise (even at rest), that have good response to short acting oral nitrates and oral calcium channel blockers (CCB)1. Some patients with VA develop malignant ventricular arrythmias during ischemic episodes that lead to sudden death2. Although VA usually has a good response to oral nitrates and oral CCB, treatment of patients that cannot tolerate oral drugs (on the acute phase of sudden death, hemodynamically unstable or patients on mechanical ventilation) options are very reduced. In this case report, we present a patient with an outpatient aborted sudden death due to VA with frequent episodes of coronary arteries vasospasms with malignant ventricular arrythmias refractory to intravenous nitrates that responded to clevidipine, an intravenous CCB. A 65-years-old male patient was brought to the emergency room due to out-of-hospital cardiac arrest. Past medical history of hypertriglyceridemia and was an active smoker. Chronic medication included atorvastatin 20 mg once daily (OD) and acetylsalicylic acid 100 mg (OD). The patient suffered cardiac arrest while traveling on public bus and basic life support maneuvers were started until medical assistance arrived. The automated external defibrillator showed a ventricular fibrillation (VF) and after 2 shocks of 200 Joules (J) and 15 min of cardiopulmonary resuscitation maneuvers the patient recovered pulse. The 12-lead electrocardiogram (ECG) showed sinus tachycardia without signs of myocardial ischemia. The patient was transferred to the hospital with mechanical ventilation support. Once on the emergency room, the patient was hemodynamically stable without vasoactive drugs. No remarkable findings on physical examination. The ECG showed a sinus tachycardia without alterations suggestive of myocardial ischemia (Fig. 1A). An emergency echocardiogram was performed and normal size non-hypertrophic left ventricle with mild global hypokinesia (no regional alterations in contraction suggestive of coronary artery disease) was found. Anyways, hemodynamics laboratory was contacted for an urgent coronarography to exclude myocardial ischemia as the cause of VF.\",\"PeriodicalId\":8360,\"journal\":{\"name\":\"Archivos de cardiologia de Mexico\",\"volume\":\"92 4\",\"pages\":\"537-540\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2022-10-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/97/aa/6936AX214-ACM-92-537.PMC9681519.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Archivos de cardiologia de Mexico\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.24875/ACM.21000251\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Archivos de cardiologia de Mexico","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.24875/ACM.21000251","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Malignant coronary vasospasm refractory to nitrates: Using clevidipine as an emergent coronary vasodilator.
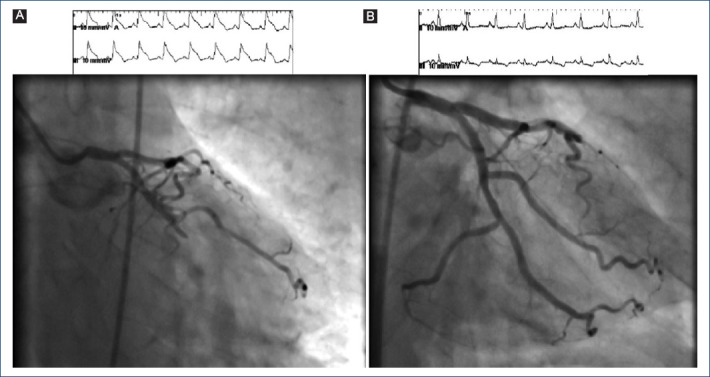
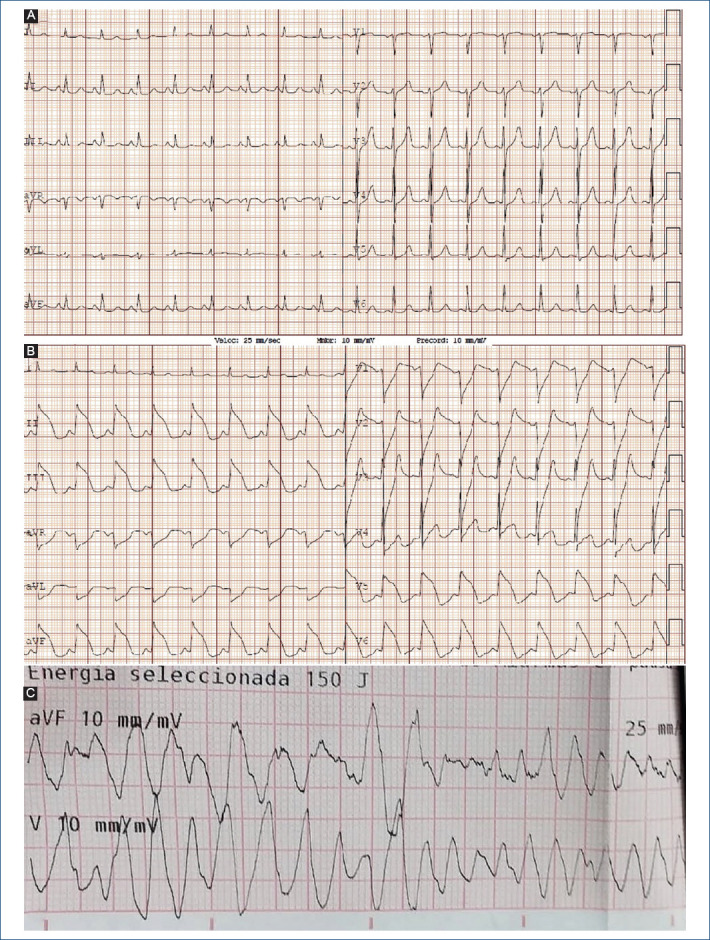
Coronary artery vasospasm is a cause of chest pain described more than 50 years ago by Prinzmetal et al., named as variant angina1. Now, it is commonly known as Prinzmetal angina or vasospastic angina (VA). Patients with VA have episodes of oppressive chest pain, characterized by diurnal variation and not with exercise (even at rest), that have good response to short acting oral nitrates and oral calcium channel blockers (CCB)1. Some patients with VA develop malignant ventricular arrythmias during ischemic episodes that lead to sudden death2. Although VA usually has a good response to oral nitrates and oral CCB, treatment of patients that cannot tolerate oral drugs (on the acute phase of sudden death, hemodynamically unstable or patients on mechanical ventilation) options are very reduced. In this case report, we present a patient with an outpatient aborted sudden death due to VA with frequent episodes of coronary arteries vasospasms with malignant ventricular arrythmias refractory to intravenous nitrates that responded to clevidipine, an intravenous CCB. A 65-years-old male patient was brought to the emergency room due to out-of-hospital cardiac arrest. Past medical history of hypertriglyceridemia and was an active smoker. Chronic medication included atorvastatin 20 mg once daily (OD) and acetylsalicylic acid 100 mg (OD). The patient suffered cardiac arrest while traveling on public bus and basic life support maneuvers were started until medical assistance arrived. The automated external defibrillator showed a ventricular fibrillation (VF) and after 2 shocks of 200 Joules (J) and 15 min of cardiopulmonary resuscitation maneuvers the patient recovered pulse. The 12-lead electrocardiogram (ECG) showed sinus tachycardia without signs of myocardial ischemia. The patient was transferred to the hospital with mechanical ventilation support. Once on the emergency room, the patient was hemodynamically stable without vasoactive drugs. No remarkable findings on physical examination. The ECG showed a sinus tachycardia without alterations suggestive of myocardial ischemia (Fig. 1A). An emergency echocardiogram was performed and normal size non-hypertrophic left ventricle with mild global hypokinesia (no regional alterations in contraction suggestive of coronary artery disease) was found. Anyways, hemodynamics laboratory was contacted for an urgent coronarography to exclude myocardial ischemia as the cause of VF.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


