{"title":"通过延长剂量间隔,实现长效注射抗精神病药物的渐进式、双曲式减量:一项计算机模拟研究。","authors":"James R O'Neill, David M Taylor, Mark A Horowitz","doi":"10.1177/20451253231198463","DOIUrl":null,"url":null,"abstract":"<p><p>Gradual, hyperbolic tapering has been proposed as a method to reduce the risk of withdrawal effects and potential relapse of an underlying condition by minimising disruption of existing equilibria. We applied hyperbolic tapering principles <i>in silico</i> to long-acting aripiprazole to generate regimens for withdrawal in clinical practice. We derived thresholds for taper rates using existing studies and consensus. Using pharmacokinetic data for aripiprazole long-acting injectable antipsychotic (ALAI), we conducted <i>in silico</i> modelling to examine the impact of abrupt cessation of long-acting injectable antipsychotic (LAI) medication and the effect of prolonging inter-dose interval on plasma aripiprazole levels and consequent D<sub>2</sub> occupancy. We also modelled transitions from LAI medication to oral medication. Regimens were designed to afford a rate of reduction between 5 and 12.5 percentage points of D<sub>2</sub> occupancy per month. Abrupt discontinuation of ALAI was shown to lead to a maximal D<sub>2</sub> occupancy reduction of 16.8 percentage points per month; prolongation of the inter-dose interval of ALAI produced a slower reduction. Specifically, hyperbolic tapering was afforded by prolongation of a 400 mg ALAI inter-dose interval from 4 to 7 weeks, before reducing the dose to 300 mg ALAI. This could then be administered at up to 4-week (for 6% maximal D<sub>2</sub> occupancy change), 6-week (9% change) or 7-week (11% change) intervals. Switching to oral medication - 5, 2.5 and 1.25 mg for the three regimens, respectively - is required for ALAI to complete full cessation to prevent too rapid a reduction in D<sub>2</sub> occupancy. Oral medication should probably be maintained at a consistent dose for 3-6 months before further reductions to account for residual LAI being concurrently eliminated. Hyperbolic dose tapering is possible with ALAI through prolongation of the inter-dose interval and may reduce the risk of relapse compared to abrupt discontinuation of LAI medication.</p>","PeriodicalId":23127,"journal":{"name":"Therapeutic Advances in Psychopharmacology","volume":"13 ","pages":"20451253231198463"},"PeriodicalIF":4.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/62/e1/10.1177_20451253231198463.PMC10501077.pdf","citationCount":"0","resultStr":"{\"title\":\"Implementing gradual, hyperbolic tapering of long-acting injectable antipsychotics by prolonging the inter-dose interval: an <i>in silico</i> modelling study.\",\"authors\":\"James R O'Neill, David M Taylor, Mark A Horowitz\",\"doi\":\"10.1177/20451253231198463\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Gradual, hyperbolic tapering has been proposed as a method to reduce the risk of withdrawal effects and potential relapse of an underlying condition by minimising disruption of existing equilibria. We applied hyperbolic tapering principles <i>in silico</i> to long-acting aripiprazole to generate regimens for withdrawal in clinical practice. We derived thresholds for taper rates using existing studies and consensus. Using pharmacokinetic data for aripiprazole long-acting injectable antipsychotic (ALAI), we conducted <i>in silico</i> modelling to examine the impact of abrupt cessation of long-acting injectable antipsychotic (LAI) medication and the effect of prolonging inter-dose interval on plasma aripiprazole levels and consequent D<sub>2</sub> occupancy. We also modelled transitions from LAI medication to oral medication. Regimens were designed to afford a rate of reduction between 5 and 12.5 percentage points of D<sub>2</sub> occupancy per month. Abrupt discontinuation of ALAI was shown to lead to a maximal D<sub>2</sub> occupancy reduction of 16.8 percentage points per month; prolongation of the inter-dose interval of ALAI produced a slower reduction. Specifically, hyperbolic tapering was afforded by prolongation of a 400 mg ALAI inter-dose interval from 4 to 7 weeks, before reducing the dose to 300 mg ALAI. This could then be administered at up to 4-week (for 6% maximal D<sub>2</sub> occupancy change), 6-week (9% change) or 7-week (11% change) intervals. Switching to oral medication - 5, 2.5 and 1.25 mg for the three regimens, respectively - is required for ALAI to complete full cessation to prevent too rapid a reduction in D<sub>2</sub> occupancy. Oral medication should probably be maintained at a consistent dose for 3-6 months before further reductions to account for residual LAI being concurrently eliminated. Hyperbolic dose tapering is possible with ALAI through prolongation of the inter-dose interval and may reduce the risk of relapse compared to abrupt discontinuation of LAI medication.</p>\",\"PeriodicalId\":23127,\"journal\":{\"name\":\"Therapeutic Advances in Psychopharmacology\",\"volume\":\"13 \",\"pages\":\"20451253231198463\"},\"PeriodicalIF\":4.0000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/62/e1/10.1177_20451253231198463.PMC10501077.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Therapeutic Advances in Psychopharmacology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/20451253231198463\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Psychopharmacology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/20451253231198463","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
Implementing gradual, hyperbolic tapering of long-acting injectable antipsychotics by prolonging the inter-dose interval: an in silico modelling study.
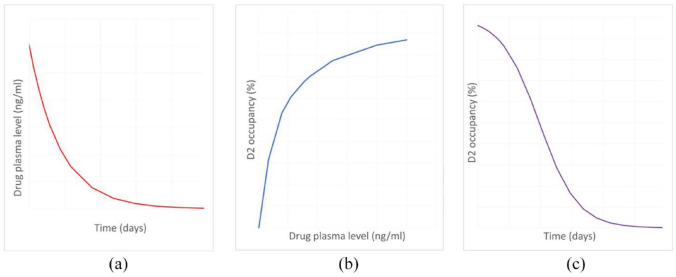
Gradual, hyperbolic tapering has been proposed as a method to reduce the risk of withdrawal effects and potential relapse of an underlying condition by minimising disruption of existing equilibria. We applied hyperbolic tapering principles in silico to long-acting aripiprazole to generate regimens for withdrawal in clinical practice. We derived thresholds for taper rates using existing studies and consensus. Using pharmacokinetic data for aripiprazole long-acting injectable antipsychotic (ALAI), we conducted in silico modelling to examine the impact of abrupt cessation of long-acting injectable antipsychotic (LAI) medication and the effect of prolonging inter-dose interval on plasma aripiprazole levels and consequent D2 occupancy. We also modelled transitions from LAI medication to oral medication. Regimens were designed to afford a rate of reduction between 5 and 12.5 percentage points of D2 occupancy per month. Abrupt discontinuation of ALAI was shown to lead to a maximal D2 occupancy reduction of 16.8 percentage points per month; prolongation of the inter-dose interval of ALAI produced a slower reduction. Specifically, hyperbolic tapering was afforded by prolongation of a 400 mg ALAI inter-dose interval from 4 to 7 weeks, before reducing the dose to 300 mg ALAI. This could then be administered at up to 4-week (for 6% maximal D2 occupancy change), 6-week (9% change) or 7-week (11% change) intervals. Switching to oral medication - 5, 2.5 and 1.25 mg for the three regimens, respectively - is required for ALAI to complete full cessation to prevent too rapid a reduction in D2 occupancy. Oral medication should probably be maintained at a consistent dose for 3-6 months before further reductions to account for residual LAI being concurrently eliminated. Hyperbolic dose tapering is possible with ALAI through prolongation of the inter-dose interval and may reduce the risk of relapse compared to abrupt discontinuation of LAI medication.
期刊介绍:
Therapeutic Advances in Psychopharmacology delivers the highest quality peer-reviewed articles, reviews, and scholarly comment on pioneering efforts and innovative studies across all areas of psychopharmacology. The journal has a strong clinical and pharmacological focus and is aimed at clinicians and researchers in psychopharmacology, providing a forum in print and online for publishing the highest quality articles in this area.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


