{"title":"我们应该在什么时候介入放射学介入治疗急性肺栓塞?","authors":"María Barca-Hernando, Luis Jara-Palomares","doi":"10.1183/20734735.0085-2023","DOIUrl":null,"url":null,"abstract":"<p><p>Pulmonary embolism (PE) is a common disease associated with high morbidity and mortality. Currently, guidelines recommend systemic thrombolysis in patients with haemodynamic instability (high-risk PE) or patients with intermediate-high-risk PE with haemodynamic deterioration. Nevertheless, more than half of high-risk PE patients do not receive systemic thrombolysis due to a perceived increased risk of bleeding. In these cases, percutaneous catheter-directed therapy (CDT) or surgical embolectomy should be considered. CDT has emerged and appears to be an effective alternative in treating PE, with a hypothetical lower risk of bleeding than systemic thrombolysis, acting directly in the thrombus with a much lower dose of thrombolytic drug or even without thrombolytic therapy. CDT techniques include catheter-directed clot aspiration or fragmentation, mechanical embolectomy, local thrombolysis, and combined pharmaco-mechanical approaches. A few observational prospective studies have demonstrated that CDT improves right ventricular function with a low rate of haemorrhage. Nevertheless, the evidence from randomised controlled trials is scarce. Here we review different scenarios where CDT may be useful and trials ongoing in this field. These results may change the upcoming guidelines for management and treatment of PE, establishing CDT as a recommended treatment in patients with acute intermediate-high-risk PE.</p>","PeriodicalId":72461,"journal":{"name":"","volume":"19 3","pages":"230085"},"PeriodicalIF":0.0,"publicationDate":"2023-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/fb/a4/EDU-0085-2023.PMC10501706.pdf","citationCount":"0","resultStr":"{\"title\":\"When should we involve interventional radiology in the management of acute pulmonary embolism?\",\"authors\":\"María Barca-Hernando, Luis Jara-Palomares\",\"doi\":\"10.1183/20734735.0085-2023\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Pulmonary embolism (PE) is a common disease associated with high morbidity and mortality. Currently, guidelines recommend systemic thrombolysis in patients with haemodynamic instability (high-risk PE) or patients with intermediate-high-risk PE with haemodynamic deterioration. Nevertheless, more than half of high-risk PE patients do not receive systemic thrombolysis due to a perceived increased risk of bleeding. In these cases, percutaneous catheter-directed therapy (CDT) or surgical embolectomy should be considered. CDT has emerged and appears to be an effective alternative in treating PE, with a hypothetical lower risk of bleeding than systemic thrombolysis, acting directly in the thrombus with a much lower dose of thrombolytic drug or even without thrombolytic therapy. CDT techniques include catheter-directed clot aspiration or fragmentation, mechanical embolectomy, local thrombolysis, and combined pharmaco-mechanical approaches. A few observational prospective studies have demonstrated that CDT improves right ventricular function with a low rate of haemorrhage. Nevertheless, the evidence from randomised controlled trials is scarce. Here we review different scenarios where CDT may be useful and trials ongoing in this field. These results may change the upcoming guidelines for management and treatment of PE, establishing CDT as a recommended treatment in patients with acute intermediate-high-risk PE.</p>\",\"PeriodicalId\":72461,\"journal\":{\"name\":\"\",\"volume\":\"19 3\",\"pages\":\"230085\"},\"PeriodicalIF\":0.0,\"publicationDate\":\"2023-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/fb/a4/EDU-0085-2023.PMC10501706.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1183/20734735.0085-2023\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/9/12 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1183/20734735.0085-2023","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/9/12 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
When should we involve interventional radiology in the management of acute pulmonary embolism?
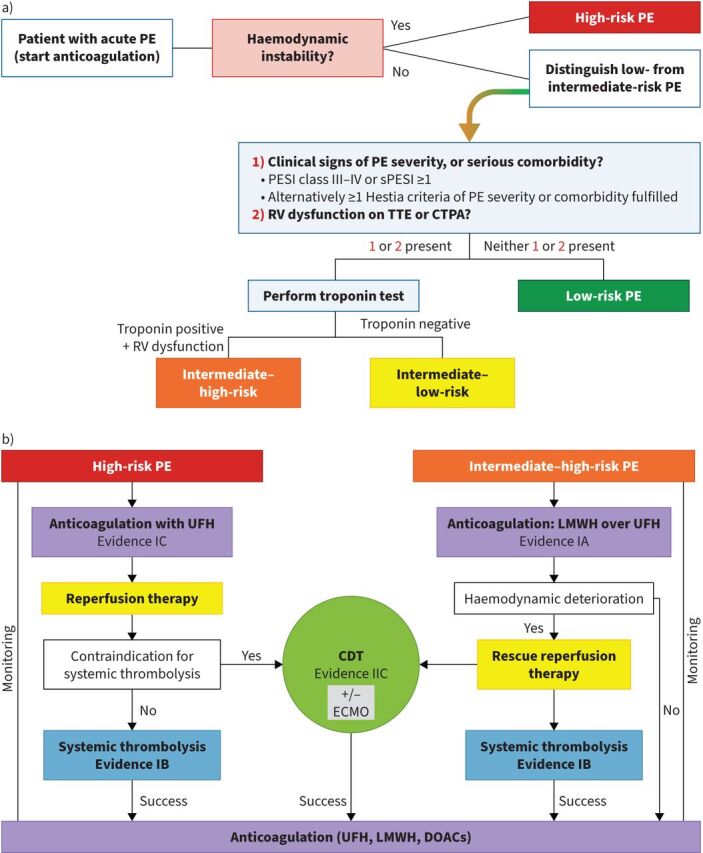
Pulmonary embolism (PE) is a common disease associated with high morbidity and mortality. Currently, guidelines recommend systemic thrombolysis in patients with haemodynamic instability (high-risk PE) or patients with intermediate-high-risk PE with haemodynamic deterioration. Nevertheless, more than half of high-risk PE patients do not receive systemic thrombolysis due to a perceived increased risk of bleeding. In these cases, percutaneous catheter-directed therapy (CDT) or surgical embolectomy should be considered. CDT has emerged and appears to be an effective alternative in treating PE, with a hypothetical lower risk of bleeding than systemic thrombolysis, acting directly in the thrombus with a much lower dose of thrombolytic drug or even without thrombolytic therapy. CDT techniques include catheter-directed clot aspiration or fragmentation, mechanical embolectomy, local thrombolysis, and combined pharmaco-mechanical approaches. A few observational prospective studies have demonstrated that CDT improves right ventricular function with a low rate of haemorrhage. Nevertheless, the evidence from randomised controlled trials is scarce. Here we review different scenarios where CDT may be useful and trials ongoing in this field. These results may change the upcoming guidelines for management and treatment of PE, establishing CDT as a recommended treatment in patients with acute intermediate-high-risk PE.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


