Offir Ukashi, Doron Yablecovitch, Adi Lahat, Limor Selinger, Sandra Neuman, Rami Eliakim, Shomron Ben-Horin, Uri Kopylov
{"title":"中段小肠Lewis评分可预测静止性克罗恩病患者的长期预后。","authors":"Offir Ukashi, Doron Yablecovitch, Adi Lahat, Limor Selinger, Sandra Neuman, Rami Eliakim, Shomron Ben-Horin, Uri Kopylov","doi":"10.1177/17562848231188587","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Video capsule endoscopy (VCE) has been proven to accurately diagnose small-bowel inflammation and predict flares among patients with quiescent Crohn's disease (CD). However, data regarding its predictive role in this population over an extended follow-up are scarce.</p><p><strong>Objectives: </strong>To predict clinical exacerbation and to assess the yield of Lewis score in identifying CD patients with future clinical exacerbation during an extended follow-up (>24 months).</p><p><strong>Design: </strong>A <i>post hoc</i> analysis study.</p><p><strong>Methods: </strong>Adult patients with quiescent small-bowel CD who were followed with VCE, inflammatory biomarkers and magnetic resonance enterography in a prospective study (between 2013 and 2018). We extracted extended clinical data (up to April 2022). The primary composite outcome (i.e. clinical exacerbation) was defined as intestinal surgery, endoscopic dilation, CD-related admission, corticosteroid administration, or biological/immunomodulator treatment change during follow-up.</p><p><strong>Results: </strong>Of the 61 patients in the study [median age 29 (24-37) years, male 57.4%, biologic treatment 46.7%], 18 patients met the primary outcome during an extended follow-up [median 58.0 (34.5-93.0) months]. On univariable analysis, complicated [hazard ratio (HR) 7.348, <i>p</i> = 0.002] and stricturing disease phenotype (HR 5.305, <i>p</i> = 0.001) were associated with higher risk for clinical exacerbation during follow-up. A baseline VCE middle small-bowel segment Lewis score (midLS) ⩾ 135 identified patients with future exacerbation [AUC (area under the curve) 0.767, 95% confidence interval (CI) 0.633-0.902, <i>p</i> = 0.001, HR 6.317, 93% negative predictive value], whereas the AUC of the conventional Lewis score was 0.734 (95% CI: 0.589-0.879, <i>p</i> = 0.004). Sensitivity analysis restricted to patients with either complicated (<i>n</i> = 34) or stricturing (<i>n</i> = 26) disease phenotype revealed that midLS still predicted clinical exacerbation during follow-up (AUC 0.747/0.753, respectively), in these patients.</p><p><strong>Conclusion: </strong>MidLS predicts treatment failure in quiescent CD patients (median follow-up of 5 years) independently of disease phenotype.</p>","PeriodicalId":23022,"journal":{"name":"Therapeutic Advances in Gastroenterology","volume":"16 ","pages":"17562848231188587"},"PeriodicalIF":3.4000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/dd/89/10.1177_17562848231188587.PMC10392190.pdf","citationCount":"0","resultStr":"{\"title\":\"Middle small-bowel segment Lewis score may predict long-term outcomes among patients with quiescent Crohn's disease.\",\"authors\":\"Offir Ukashi, Doron Yablecovitch, Adi Lahat, Limor Selinger, Sandra Neuman, Rami Eliakim, Shomron Ben-Horin, Uri Kopylov\",\"doi\":\"10.1177/17562848231188587\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Video capsule endoscopy (VCE) has been proven to accurately diagnose small-bowel inflammation and predict flares among patients with quiescent Crohn's disease (CD). However, data regarding its predictive role in this population over an extended follow-up are scarce.</p><p><strong>Objectives: </strong>To predict clinical exacerbation and to assess the yield of Lewis score in identifying CD patients with future clinical exacerbation during an extended follow-up (>24 months).</p><p><strong>Design: </strong>A <i>post hoc</i> analysis study.</p><p><strong>Methods: </strong>Adult patients with quiescent small-bowel CD who were followed with VCE, inflammatory biomarkers and magnetic resonance enterography in a prospective study (between 2013 and 2018). We extracted extended clinical data (up to April 2022). The primary composite outcome (i.e. clinical exacerbation) was defined as intestinal surgery, endoscopic dilation, CD-related admission, corticosteroid administration, or biological/immunomodulator treatment change during follow-up.</p><p><strong>Results: </strong>Of the 61 patients in the study [median age 29 (24-37) years, male 57.4%, biologic treatment 46.7%], 18 patients met the primary outcome during an extended follow-up [median 58.0 (34.5-93.0) months]. On univariable analysis, complicated [hazard ratio (HR) 7.348, <i>p</i> = 0.002] and stricturing disease phenotype (HR 5.305, <i>p</i> = 0.001) were associated with higher risk for clinical exacerbation during follow-up. A baseline VCE middle small-bowel segment Lewis score (midLS) ⩾ 135 identified patients with future exacerbation [AUC (area under the curve) 0.767, 95% confidence interval (CI) 0.633-0.902, <i>p</i> = 0.001, HR 6.317, 93% negative predictive value], whereas the AUC of the conventional Lewis score was 0.734 (95% CI: 0.589-0.879, <i>p</i> = 0.004). Sensitivity analysis restricted to patients with either complicated (<i>n</i> = 34) or stricturing (<i>n</i> = 26) disease phenotype revealed that midLS still predicted clinical exacerbation during follow-up (AUC 0.747/0.753, respectively), in these patients.</p><p><strong>Conclusion: </strong>MidLS predicts treatment failure in quiescent CD patients (median follow-up of 5 years) independently of disease phenotype.</p>\",\"PeriodicalId\":23022,\"journal\":{\"name\":\"Therapeutic Advances in Gastroenterology\",\"volume\":\"16 \",\"pages\":\"17562848231188587\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/dd/89/10.1177_17562848231188587.PMC10392190.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Therapeutic Advances in Gastroenterology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/17562848231188587\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Gastroenterology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/17562848231188587","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:视频胶囊内窥镜(VCE)已被证明可以准确诊断静止性克罗恩病(CD)患者的小肠炎症并预测其发作。然而,在长期随访中,关于其在该人群中的预测作用的数据很少。目的:在延长随访(>24个月)期间,预测临床恶化,并评估Lewis评分在识别CD患者未来临床恶化中的分值。设计:一项事后分析研究。方法:在一项前瞻性研究中(2013年至2018年),对成年静态小肠CD患者进行VCE、炎症生物标志物和磁共振肠造影随访。我们提取了延伸的临床数据(截至2022年4月)。主要复合结局(即临床恶化)被定义为肠道手术、内镜扩张、cd相关入院、皮质类固醇治疗或随访期间生物/免疫调节剂治疗的改变。结果:在研究的61例患者中[中位年龄29(24-37)岁,男性57.4%,生物治疗46.7%],18例患者在延长随访期间达到主要结局[中位58.0(34.5-93.0)个月]。单变量分析显示,复杂[危险比(HR) 7.348, p = 0.002]和狭窄性疾病表型(HR 5.305, p = 0.001)与随访期间临床恶化的高风险相关。基线VCE中小肠段Lewis评分(midLS)大于或等于135确定了未来恶化的患者[AUC(曲线下面积)0.767,95%可信区间(CI) 0.633-0.902, p = 0.001, HR 6.317, 93%阴性预测值],而传统Lewis评分的AUC为0.734 (95% CI: 0.589-0.879, p = 0.004)。对复杂(n = 34)或狭窄(n = 26)疾病表型患者的敏感性分析显示,在这些患者中,随访期间midLS仍然预测临床恶化(AUC分别为0.747/0.753)。结论:MidLS预测静止期CD患者(中位随访5年)治疗失败与疾病表型无关。
Middle small-bowel segment Lewis score may predict long-term outcomes among patients with quiescent Crohn's disease.
Background: Video capsule endoscopy (VCE) has been proven to accurately diagnose small-bowel inflammation and predict flares among patients with quiescent Crohn's disease (CD). However, data regarding its predictive role in this population over an extended follow-up are scarce.
Objectives: To predict clinical exacerbation and to assess the yield of Lewis score in identifying CD patients with future clinical exacerbation during an extended follow-up (>24 months).
Design: A post hoc analysis study.
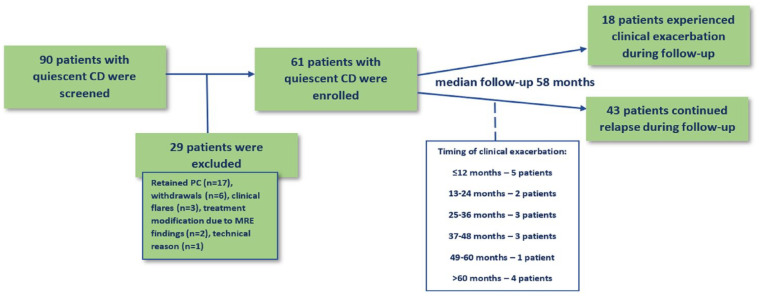
Methods: Adult patients with quiescent small-bowel CD who were followed with VCE, inflammatory biomarkers and magnetic resonance enterography in a prospective study (between 2013 and 2018). We extracted extended clinical data (up to April 2022). The primary composite outcome (i.e. clinical exacerbation) was defined as intestinal surgery, endoscopic dilation, CD-related admission, corticosteroid administration, or biological/immunomodulator treatment change during follow-up.
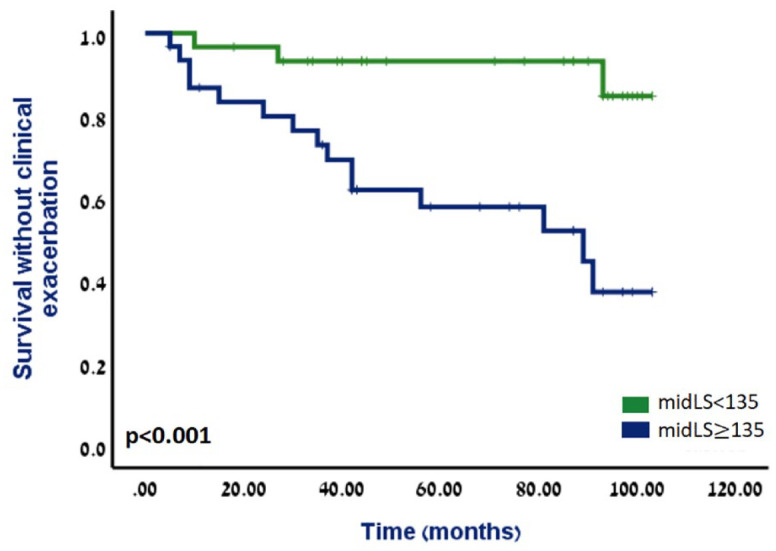
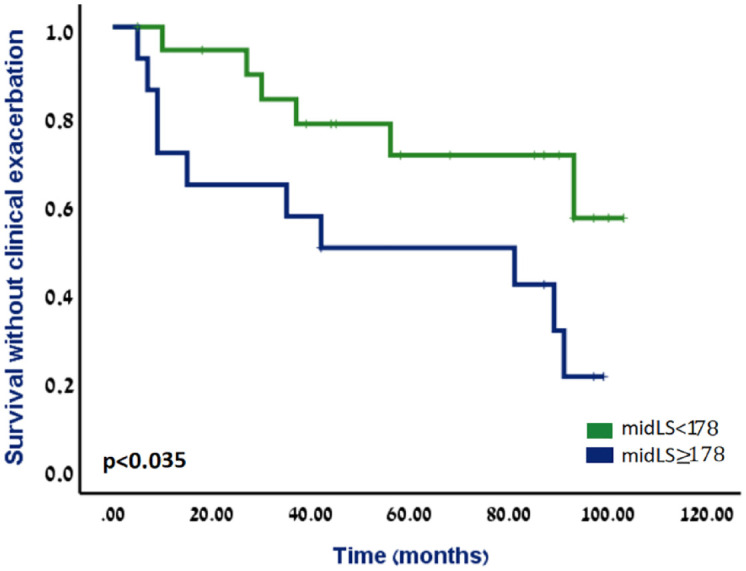
Results: Of the 61 patients in the study [median age 29 (24-37) years, male 57.4%, biologic treatment 46.7%], 18 patients met the primary outcome during an extended follow-up [median 58.0 (34.5-93.0) months]. On univariable analysis, complicated [hazard ratio (HR) 7.348, p = 0.002] and stricturing disease phenotype (HR 5.305, p = 0.001) were associated with higher risk for clinical exacerbation during follow-up. A baseline VCE middle small-bowel segment Lewis score (midLS) ⩾ 135 identified patients with future exacerbation [AUC (area under the curve) 0.767, 95% confidence interval (CI) 0.633-0.902, p = 0.001, HR 6.317, 93% negative predictive value], whereas the AUC of the conventional Lewis score was 0.734 (95% CI: 0.589-0.879, p = 0.004). Sensitivity analysis restricted to patients with either complicated (n = 34) or stricturing (n = 26) disease phenotype revealed that midLS still predicted clinical exacerbation during follow-up (AUC 0.747/0.753, respectively), in these patients.
Conclusion: MidLS predicts treatment failure in quiescent CD patients (median follow-up of 5 years) independently of disease phenotype.
期刊介绍:
Therapeutic Advances in Gastroenterology is an open access journal which delivers the highest quality peer-reviewed original research articles, reviews, and scholarly comment on pioneering efforts and innovative studies in the medical treatment of gastrointestinal and hepatic disorders. The journal has a strong clinical and pharmacological focus and is aimed at an international audience of clinicians and researchers in gastroenterology and related disciplines, providing an online forum for rapid dissemination of recent research and perspectives in this area.
The editors welcome original research articles across all areas of gastroenterology and hepatology.
The journal publishes original research articles and review articles primarily. Original research manuscripts may include laboratory, animal or human/clinical studies – all phases. Letters to the Editor and Case Reports will also be considered.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


