{"title":"COVID-19的最佳抗凝策略是预防性还是治疗性?:对超过27000名参与者进行了荟萃分析、试验序列分析和荟萃回归。","authors":"Mingyue Guo, Qi Han, Jiaxuan Xing, Feng Xu, Jiali Wang, Chuanbao Li, Zechen Shan, Yuan Bian, Hao Wang, Li Xue, Qiuhuan Yuan, Chang Pan, Yanshan De, Xingfang Wang, Panpan Hao, Shengchuan Cao, Jiaojiao Pang, Yuguo Chen","doi":"10.1097/EC9.0000000000000059","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Anticoagulants are promising regimens for treating coronavirus disease 2019 (COVID-19). However, whether prophylactic or intermediate-to-therapeutic dosage is optimal remains under active discussion.</p><p><strong>Methods: </strong>We comprehensively searched PubMed, Embase, Scopus, Web of Science, Cochrane Library, ClinicalTrials, and MedRxiv databases on April 26, 2022. Two independent researchers conducted literature selection and data extraction separately according to predetermined criteria. Notably, this is the first meta-analysis on COVID-19, taking serious consideration regarding the dosage overlap between the 2 comparison groups of prophylactic anticoagulation (PA) and intermediate-to-therapeutic anticoagulation (I-TA).</p><p><strong>Results: </strong>We included 11 randomized controlled trials (RCTs) and 36 cohort studies with 27,051 COVID-19 patients. By analyzing all the RCTs, there was no significant difference in mortality between the PA and I-TA groups, which was further confirmed by trial sequential analysis (TSA) (odds ratio [OR]: 0.93; 95% confidence interval [CI]: 0.71-1.22; <i>P</i> = 0.61; TSA adjusted CI: 0.71-1.26). The rate of major bleeding was remarkably higher in the I-TA group than in the PA group, despite adjusting for TSA (OR: 1.73; 95% CI: 1.15-2.60; <i>P</i> = 0.009; TSA adjusted CI: 1.09-2.58). RCTs have supported the beneficial effect of I-TA in reducing thrombotic events. After including all studies, mortality in the I-TA group was significantly higher than in the PA group (OR: 1.38; 95% CI: 1.15-1.66; <i>P</i> = 0.0005). The rate of major bleeding was similar to the analysis from RCTs (OR: 2.24; 95% CI: 1.86-2.69; <i>P</i> < 0.00001). There was no distinct difference in the rate of thrombotic events between the 2 regimen groups. In addition, in both critical and noncritical subgroups, I-TA failed to reduce mortality but increased major bleeding rate compared with PA, as shown in meta-analysis of all studies, as well as RCTs only. Meta-regression of all studies suggested that there was no relationship between the treatment effect and the overall risk of mortality or major bleeding (<i>P</i> = 0.14, <i>P</i> = 0.09, respectively).</p><p><strong>Conclusion: </strong>I-TA is not superior to PA for treating COVID-19 because it fails to lower the mortality rate but increases the major bleeding rate in both critical and noncritical patients.</p>","PeriodicalId":72895,"journal":{"name":"Emergency and critical care medicine","volume":"2 3","pages":"148-166"},"PeriodicalIF":0.0000,"publicationDate":"2022-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/9f/be/eccm-2-148.PMC9555559.pdf","citationCount":"0","resultStr":"{\"title\":\"The optimal anticoagulation strategy for COVID-19, prophylactic or therapeutic?: a meta-analysis, trial sequential analysis, and meta-regression of more than 27,000 participants.\",\"authors\":\"Mingyue Guo, Qi Han, Jiaxuan Xing, Feng Xu, Jiali Wang, Chuanbao Li, Zechen Shan, Yuan Bian, Hao Wang, Li Xue, Qiuhuan Yuan, Chang Pan, Yanshan De, Xingfang Wang, Panpan Hao, Shengchuan Cao, Jiaojiao Pang, Yuguo Chen\",\"doi\":\"10.1097/EC9.0000000000000059\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Anticoagulants are promising regimens for treating coronavirus disease 2019 (COVID-19). However, whether prophylactic or intermediate-to-therapeutic dosage is optimal remains under active discussion.</p><p><strong>Methods: </strong>We comprehensively searched PubMed, Embase, Scopus, Web of Science, Cochrane Library, ClinicalTrials, and MedRxiv databases on April 26, 2022. Two independent researchers conducted literature selection and data extraction separately according to predetermined criteria. Notably, this is the first meta-analysis on COVID-19, taking serious consideration regarding the dosage overlap between the 2 comparison groups of prophylactic anticoagulation (PA) and intermediate-to-therapeutic anticoagulation (I-TA).</p><p><strong>Results: </strong>We included 11 randomized controlled trials (RCTs) and 36 cohort studies with 27,051 COVID-19 patients. By analyzing all the RCTs, there was no significant difference in mortality between the PA and I-TA groups, which was further confirmed by trial sequential analysis (TSA) (odds ratio [OR]: 0.93; 95% confidence interval [CI]: 0.71-1.22; <i>P</i> = 0.61; TSA adjusted CI: 0.71-1.26). The rate of major bleeding was remarkably higher in the I-TA group than in the PA group, despite adjusting for TSA (OR: 1.73; 95% CI: 1.15-2.60; <i>P</i> = 0.009; TSA adjusted CI: 1.09-2.58). RCTs have supported the beneficial effect of I-TA in reducing thrombotic events. After including all studies, mortality in the I-TA group was significantly higher than in the PA group (OR: 1.38; 95% CI: 1.15-1.66; <i>P</i> = 0.0005). The rate of major bleeding was similar to the analysis from RCTs (OR: 2.24; 95% CI: 1.86-2.69; <i>P</i> < 0.00001). There was no distinct difference in the rate of thrombotic events between the 2 regimen groups. In addition, in both critical and noncritical subgroups, I-TA failed to reduce mortality but increased major bleeding rate compared with PA, as shown in meta-analysis of all studies, as well as RCTs only. Meta-regression of all studies suggested that there was no relationship between the treatment effect and the overall risk of mortality or major bleeding (<i>P</i> = 0.14, <i>P</i> = 0.09, respectively).</p><p><strong>Conclusion: </strong>I-TA is not superior to PA for treating COVID-19 because it fails to lower the mortality rate but increases the major bleeding rate in both critical and noncritical patients.</p>\",\"PeriodicalId\":72895,\"journal\":{\"name\":\"Emergency and critical care medicine\",\"volume\":\"2 3\",\"pages\":\"148-166\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/9f/be/eccm-2-148.PMC9555559.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Emergency and critical care medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/EC9.0000000000000059\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/9/16 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Emergency and critical care medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/EC9.0000000000000059","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/9/16 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:抗凝剂是治疗2019冠状病毒病(COVID-19)的有希望的方案。然而,预防或中间治疗剂量是否最佳仍在积极讨论中。方法:我们于2022年4月26日全面检索PubMed、Embase、Scopus、Web of Science、Cochrane Library、ClinicalTrials和MedRxiv数据库。两名独立研究人员根据预先确定的标准分别进行文献选择和数据提取。值得注意的是,这是第一个关于COVID-19的荟萃分析,认真考虑了预防性抗凝(PA)和中间治疗性抗凝(I-TA)两个对照组之间的剂量重叠。结果:我们纳入了11项随机对照试验(RCTs)和36项队列研究,共纳入27,051例COVID-19患者。通过对所有rct的分析,PA组和I-TA组的死亡率无显著差异,试验序列分析(TSA)进一步证实了这一点(优势比[OR]: 0.93; 95%可信区间[CI]: 0.71-1.22; P = 0.61; TSA校正CI: 0.71-1.26)。经TSA校正后,I-TA组大出血率明显高于PA组(OR: 1.73; 95% CI: 1.15-2.60; P = 0.009; TSA校正CI: 1.09-2.58)。随机对照试验支持I-TA在减少血栓事件中的有益作用。纳入所有研究后,I-TA组的死亡率显著高于PA组(OR: 1.38; 95% CI: 1.15-1.66; P = 0.0005)。大出血率与rct分析相似(OR: 2.24; 95% CI: 1.86-2.69; P < 0.00001)。两种方案组之间血栓事件发生率无明显差异。此外,在关键和非关键亚组中,与PA相比,I-TA未能降低死亡率,但增加了大出血率,这在所有研究的荟萃分析中都显示出来,也只有随机对照试验。所有研究的荟萃回归显示,治疗效果与总死亡率或大出血风险之间没有关系(P = 0.14, P = 0.09)。结论:I-TA治疗COVID-19并不优于PA,其在危重和非危重患者中均未能降低病死率,但增加了大出血率。
The optimal anticoagulation strategy for COVID-19, prophylactic or therapeutic?: a meta-analysis, trial sequential analysis, and meta-regression of more than 27,000 participants.
Background: Anticoagulants are promising regimens for treating coronavirus disease 2019 (COVID-19). However, whether prophylactic or intermediate-to-therapeutic dosage is optimal remains under active discussion.
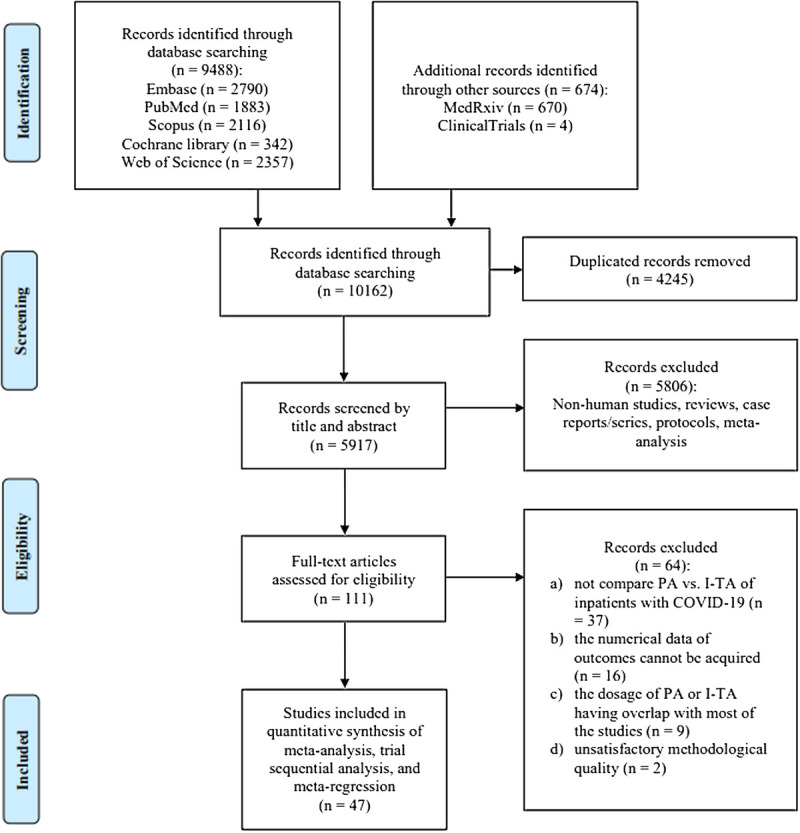
Methods: We comprehensively searched PubMed, Embase, Scopus, Web of Science, Cochrane Library, ClinicalTrials, and MedRxiv databases on April 26, 2022. Two independent researchers conducted literature selection and data extraction separately according to predetermined criteria. Notably, this is the first meta-analysis on COVID-19, taking serious consideration regarding the dosage overlap between the 2 comparison groups of prophylactic anticoagulation (PA) and intermediate-to-therapeutic anticoagulation (I-TA).
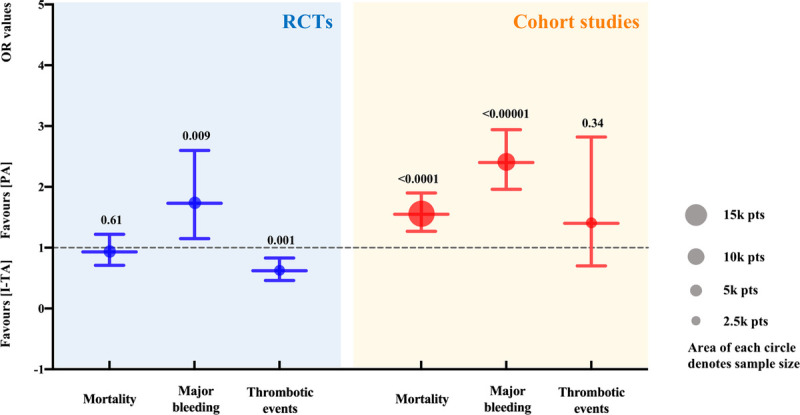
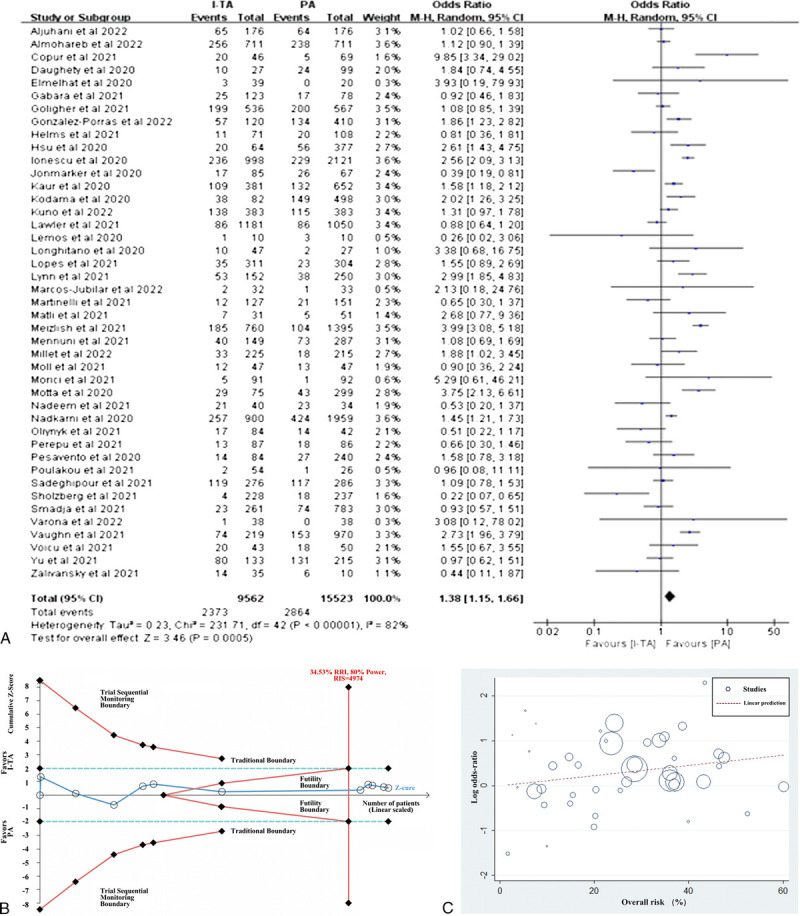
Results: We included 11 randomized controlled trials (RCTs) and 36 cohort studies with 27,051 COVID-19 patients. By analyzing all the RCTs, there was no significant difference in mortality between the PA and I-TA groups, which was further confirmed by trial sequential analysis (TSA) (odds ratio [OR]: 0.93; 95% confidence interval [CI]: 0.71-1.22; P = 0.61; TSA adjusted CI: 0.71-1.26). The rate of major bleeding was remarkably higher in the I-TA group than in the PA group, despite adjusting for TSA (OR: 1.73; 95% CI: 1.15-2.60; P = 0.009; TSA adjusted CI: 1.09-2.58). RCTs have supported the beneficial effect of I-TA in reducing thrombotic events. After including all studies, mortality in the I-TA group was significantly higher than in the PA group (OR: 1.38; 95% CI: 1.15-1.66; P = 0.0005). The rate of major bleeding was similar to the analysis from RCTs (OR: 2.24; 95% CI: 1.86-2.69; P < 0.00001). There was no distinct difference in the rate of thrombotic events between the 2 regimen groups. In addition, in both critical and noncritical subgroups, I-TA failed to reduce mortality but increased major bleeding rate compared with PA, as shown in meta-analysis of all studies, as well as RCTs only. Meta-regression of all studies suggested that there was no relationship between the treatment effect and the overall risk of mortality or major bleeding (P = 0.14, P = 0.09, respectively).
Conclusion: I-TA is not superior to PA for treating COVID-19 because it fails to lower the mortality rate but increases the major bleeding rate in both critical and noncritical patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


