Jai Mehrotra-Varma, Anand Kumthekar, Sonya Henry, Roman Fleysher, Wei Hou, Tim Q Duong
{"title":"类风湿性关节炎患者COVID-19的住院、危重疾病和死亡率结局","authors":"Jai Mehrotra-Varma, Anand Kumthekar, Sonya Henry, Roman Fleysher, Wei Hou, Tim Q Duong","doi":"10.1002/acr2.11580","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To investigate the clinical outcomes of patients with rheumatoid arthritis (RA) with COVID-19.</p><p><strong>Methods: </strong>This retrospective study consisted of 361 patients with RA+ and 45,954 patients with RA- (March 2020 to August 2022) who tested positive for SARS-CoV-2 by polymerase-chain-reaction in the Montefiore Health System, which serves a large low-income, minority-predominant population in the Bronx and was an epicenter of the initial pandemic and subsequent surges. Primary outcomes were hospitalization, critical illness, and all-cause mortality associated with SARS-CoV-2 infection. Comparisons were made with and without adjustment for covariates, as well as with 1083 matched controls of patients with RA- and COVID-19.</p><p><strong>Results: </strong>Patients with RA+ and COVID-19 were older (62.2 ± 23.5 vs. 45.5 ± 26.3; P < 0.001), were more likely females (83.1% vs. 55.8%; P < 0.001), were Black (35.5% vs. 30.3%; P < 0.05), and had higher rates of comorbidities (P < 0.05), hospitalization (52.4% vs. 32.5%; P < 0.005), critical illness (10.5% vs. 6.9%; P < 0.05), and mortality (11.1% vs. 6.2%; P < 0.01) compared with patients with RA- and COVID-19. Patients with RA+ with COVID-19 had higher odds of critical illness (adjusted odds ratio [aOR] = 1.46, 95% confidence interval [CI]: 1.09-1.93; P = 0.008) but no differences in hospitalization (aOR = 1.18 [95% CI: 0.93-1.49]; P = 0.16) and mortality (aOR = 1.34 [95% CI: 0.92-1.89]; P = 0.10) after adjusting for covariates. Odds ratio analysis identified age, hospitalization status, female sex, chronic kidney disease, chronic obstructive pulmonary disease, and Black race to be significant risk factors for COVID-19-related mortality. Pre-COVID-19 steroid and biologic therapy to treat RA were not significantly associated with worse outcomes (P > 0.05). Outcomes were not different between patients with RA+ and propensity-matched RA- controls (P > 0.05).</p><p><strong>Conclusion: </strong>Our findings suggest that risk factors for adverse COVID-19 outcomes were not attributed to RA per se but rather age and preexisting medical conditions of patients with RA.</p>","PeriodicalId":7084,"journal":{"name":"ACR Open Rheumatology","volume":"5 9","pages":"465-473"},"PeriodicalIF":0.0000,"publicationDate":"2023-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/71/4e/ACR2-5-465.PMC10502846.pdf","citationCount":"0","resultStr":"{\"title\":\"Hospitalization, Critical Illness, and Mortality Outcomes of COVID-19 in Patients With Rheumatoid Arthritis.\",\"authors\":\"Jai Mehrotra-Varma, Anand Kumthekar, Sonya Henry, Roman Fleysher, Wei Hou, Tim Q Duong\",\"doi\":\"10.1002/acr2.11580\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To investigate the clinical outcomes of patients with rheumatoid arthritis (RA) with COVID-19.</p><p><strong>Methods: </strong>This retrospective study consisted of 361 patients with RA+ and 45,954 patients with RA- (March 2020 to August 2022) who tested positive for SARS-CoV-2 by polymerase-chain-reaction in the Montefiore Health System, which serves a large low-income, minority-predominant population in the Bronx and was an epicenter of the initial pandemic and subsequent surges. Primary outcomes were hospitalization, critical illness, and all-cause mortality associated with SARS-CoV-2 infection. Comparisons were made with and without adjustment for covariates, as well as with 1083 matched controls of patients with RA- and COVID-19.</p><p><strong>Results: </strong>Patients with RA+ and COVID-19 were older (62.2 ± 23.5 vs. 45.5 ± 26.3; P < 0.001), were more likely females (83.1% vs. 55.8%; P < 0.001), were Black (35.5% vs. 30.3%; P < 0.05), and had higher rates of comorbidities (P < 0.05), hospitalization (52.4% vs. 32.5%; P < 0.005), critical illness (10.5% vs. 6.9%; P < 0.05), and mortality (11.1% vs. 6.2%; P < 0.01) compared with patients with RA- and COVID-19. Patients with RA+ with COVID-19 had higher odds of critical illness (adjusted odds ratio [aOR] = 1.46, 95% confidence interval [CI]: 1.09-1.93; P = 0.008) but no differences in hospitalization (aOR = 1.18 [95% CI: 0.93-1.49]; P = 0.16) and mortality (aOR = 1.34 [95% CI: 0.92-1.89]; P = 0.10) after adjusting for covariates. Odds ratio analysis identified age, hospitalization status, female sex, chronic kidney disease, chronic obstructive pulmonary disease, and Black race to be significant risk factors for COVID-19-related mortality. Pre-COVID-19 steroid and biologic therapy to treat RA were not significantly associated with worse outcomes (P > 0.05). Outcomes were not different between patients with RA+ and propensity-matched RA- controls (P > 0.05).</p><p><strong>Conclusion: </strong>Our findings suggest that risk factors for adverse COVID-19 outcomes were not attributed to RA per se but rather age and preexisting medical conditions of patients with RA.</p>\",\"PeriodicalId\":7084,\"journal\":{\"name\":\"ACR Open Rheumatology\",\"volume\":\"5 9\",\"pages\":\"465-473\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/71/4e/ACR2-5-465.PMC10502846.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ACR Open Rheumatology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1002/acr2.11580\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ACR Open Rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1002/acr2.11580","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Hospitalization, Critical Illness, and Mortality Outcomes of COVID-19 in Patients With Rheumatoid Arthritis.
Objective: To investigate the clinical outcomes of patients with rheumatoid arthritis (RA) with COVID-19.
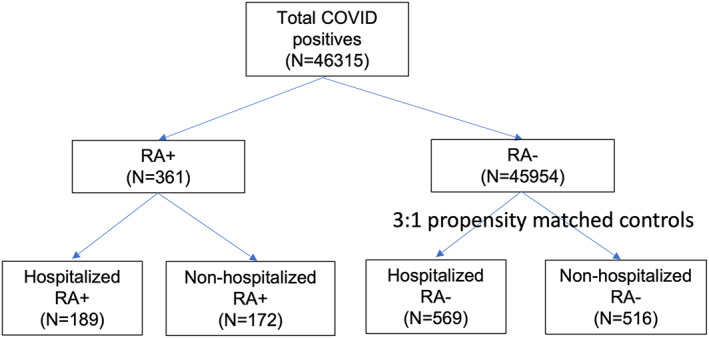
Methods: This retrospective study consisted of 361 patients with RA+ and 45,954 patients with RA- (March 2020 to August 2022) who tested positive for SARS-CoV-2 by polymerase-chain-reaction in the Montefiore Health System, which serves a large low-income, minority-predominant population in the Bronx and was an epicenter of the initial pandemic and subsequent surges. Primary outcomes were hospitalization, critical illness, and all-cause mortality associated with SARS-CoV-2 infection. Comparisons were made with and without adjustment for covariates, as well as with 1083 matched controls of patients with RA- and COVID-19.
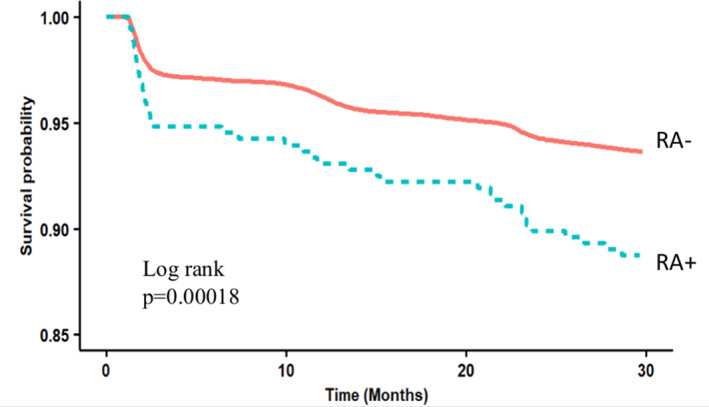
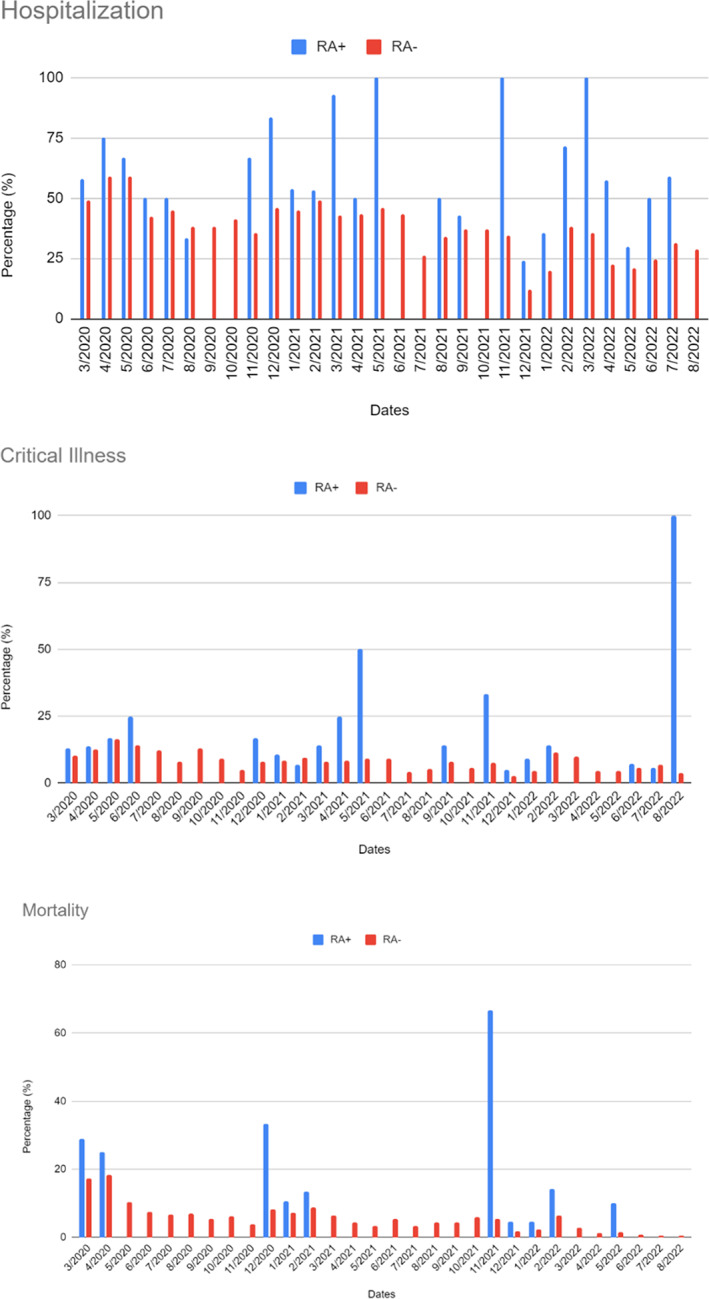
Results: Patients with RA+ and COVID-19 were older (62.2 ± 23.5 vs. 45.5 ± 26.3; P < 0.001), were more likely females (83.1% vs. 55.8%; P < 0.001), were Black (35.5% vs. 30.3%; P < 0.05), and had higher rates of comorbidities (P < 0.05), hospitalization (52.4% vs. 32.5%; P < 0.005), critical illness (10.5% vs. 6.9%; P < 0.05), and mortality (11.1% vs. 6.2%; P < 0.01) compared with patients with RA- and COVID-19. Patients with RA+ with COVID-19 had higher odds of critical illness (adjusted odds ratio [aOR] = 1.46, 95% confidence interval [CI]: 1.09-1.93; P = 0.008) but no differences in hospitalization (aOR = 1.18 [95% CI: 0.93-1.49]; P = 0.16) and mortality (aOR = 1.34 [95% CI: 0.92-1.89]; P = 0.10) after adjusting for covariates. Odds ratio analysis identified age, hospitalization status, female sex, chronic kidney disease, chronic obstructive pulmonary disease, and Black race to be significant risk factors for COVID-19-related mortality. Pre-COVID-19 steroid and biologic therapy to treat RA were not significantly associated with worse outcomes (P > 0.05). Outcomes were not different between patients with RA+ and propensity-matched RA- controls (P > 0.05).
Conclusion: Our findings suggest that risk factors for adverse COVID-19 outcomes were not attributed to RA per se but rather age and preexisting medical conditions of patients with RA.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


