Umberto Volta, Julio Cesar Bai, Roberto De Giorgio
{"title":"血清在乳糜泻诊断中的作用。","authors":"Umberto Volta, Julio Cesar Bai, Roberto De Giorgio","doi":"10.22037/ghfbb.v16i2.2713","DOIUrl":null,"url":null,"abstract":"<p><p>Serology has significantly revolutionized the knowledge of celiac disease (CD), leading to the identification of unsuspected patients in at-risk CD groups, thereby increasing the number of CD diagnoses compared to the pre-screening era. Several markers for CD with a progressive diagnostic accuracy have been identified over the years, but only three of them, i.e. anti-tissue transglutaminase (anti-tTG), anti-endomysial (EmA) and anti-deamidated gliadin antibodies (DGP) are currently assessed in the daily clinical practice. A thorough review of the literature identified 44 original studies published between 1998 to 2022 for a total of 5098 pediatric and adult CD patients (without selective IgA deficiency) and 11930 disease controls. The results highlighted that anti-tTG IgA exhibited a higher sensitivity for CD (93.4%) than EmA IgA (92.8%), DGP IgG (81.8%) and DGP IgA (83.8%). The specificity of EmA IgA (99%) resulted to be higher than those of anti-tTG IgA (95.8%), DGP IgG (96.4%) and DGP IgA (92.1%). In patients with selective IgA deficiency, a condition closely related to CD, serological screening should include one of the three antibodies of IgG class, since anti-tTG, DGP and EmA have a very similar diagnostic accuracy in this clinical setting. According to age, there are two main diagnostic strategies for CD detection. In children, the revised ESPGHAN 2020 guidelines established that CD could be diagnosed in both symptomatic and asymptomatic children by high anti-tTG IgA titers (>10 times the cut-off) and EmA positivity with no need to obtain duodenal biopsy and HLA typing. In adult patients, although high tTG IgA titers (confirmed by EmA IgA positivity) correlate with villous atrophy, an intestinal biopsy is still considered mandatory for confirming CD diagnosis. Currently, a case finding approach in at-risk groups is preferred to mass screening for CD detection.</p>","PeriodicalId":12636,"journal":{"name":"Gastroenterology and Hepatology From Bed to Bench","volume":"16 2","pages":"118-128"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/49/00/GHFBB-16-118.PMC10404833.pdf","citationCount":"0","resultStr":"{\"title\":\"The role of serology in the diagnosis of coeliac disease.\",\"authors\":\"Umberto Volta, Julio Cesar Bai, Roberto De Giorgio\",\"doi\":\"10.22037/ghfbb.v16i2.2713\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Serology has significantly revolutionized the knowledge of celiac disease (CD), leading to the identification of unsuspected patients in at-risk CD groups, thereby increasing the number of CD diagnoses compared to the pre-screening era. Several markers for CD with a progressive diagnostic accuracy have been identified over the years, but only three of them, i.e. anti-tissue transglutaminase (anti-tTG), anti-endomysial (EmA) and anti-deamidated gliadin antibodies (DGP) are currently assessed in the daily clinical practice. A thorough review of the literature identified 44 original studies published between 1998 to 2022 for a total of 5098 pediatric and adult CD patients (without selective IgA deficiency) and 11930 disease controls. The results highlighted that anti-tTG IgA exhibited a higher sensitivity for CD (93.4%) than EmA IgA (92.8%), DGP IgG (81.8%) and DGP IgA (83.8%). The specificity of EmA IgA (99%) resulted to be higher than those of anti-tTG IgA (95.8%), DGP IgG (96.4%) and DGP IgA (92.1%). In patients with selective IgA deficiency, a condition closely related to CD, serological screening should include one of the three antibodies of IgG class, since anti-tTG, DGP and EmA have a very similar diagnostic accuracy in this clinical setting. According to age, there are two main diagnostic strategies for CD detection. In children, the revised ESPGHAN 2020 guidelines established that CD could be diagnosed in both symptomatic and asymptomatic children by high anti-tTG IgA titers (>10 times the cut-off) and EmA positivity with no need to obtain duodenal biopsy and HLA typing. In adult patients, although high tTG IgA titers (confirmed by EmA IgA positivity) correlate with villous atrophy, an intestinal biopsy is still considered mandatory for confirming CD diagnosis. Currently, a case finding approach in at-risk groups is preferred to mass screening for CD detection.</p>\",\"PeriodicalId\":12636,\"journal\":{\"name\":\"Gastroenterology and Hepatology From Bed to Bench\",\"volume\":\"16 2\",\"pages\":\"118-128\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/49/00/GHFBB-16-118.PMC10404833.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Gastroenterology and Hepatology From Bed to Bench\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.22037/ghfbb.v16i2.2713\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gastroenterology and Hepatology From Bed to Bench","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22037/ghfbb.v16i2.2713","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
The role of serology in the diagnosis of coeliac disease.
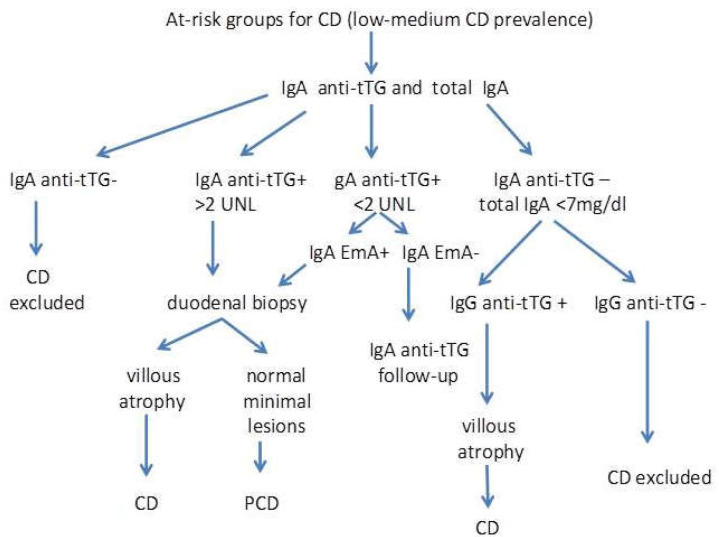
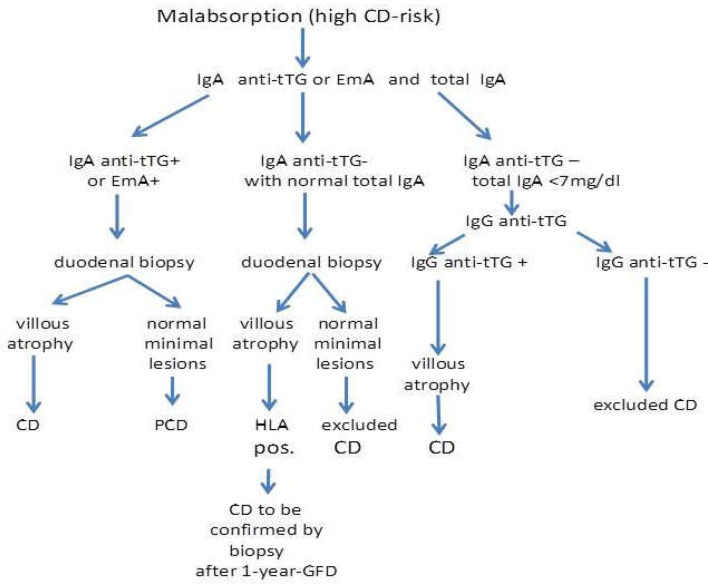
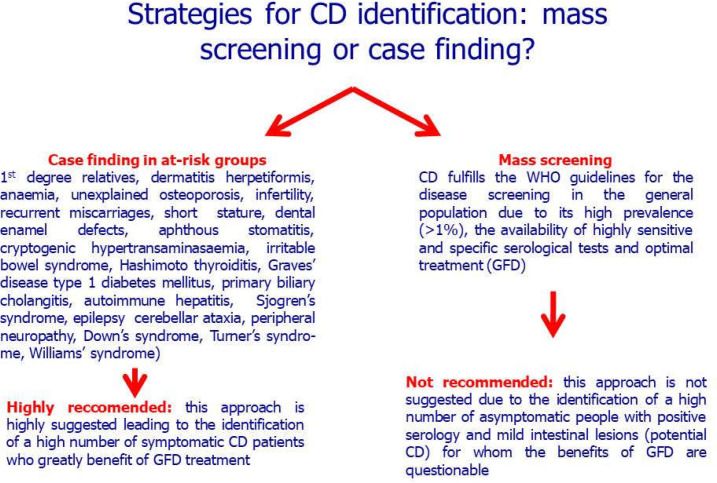
Serology has significantly revolutionized the knowledge of celiac disease (CD), leading to the identification of unsuspected patients in at-risk CD groups, thereby increasing the number of CD diagnoses compared to the pre-screening era. Several markers for CD with a progressive diagnostic accuracy have been identified over the years, but only three of them, i.e. anti-tissue transglutaminase (anti-tTG), anti-endomysial (EmA) and anti-deamidated gliadin antibodies (DGP) are currently assessed in the daily clinical practice. A thorough review of the literature identified 44 original studies published between 1998 to 2022 for a total of 5098 pediatric and adult CD patients (without selective IgA deficiency) and 11930 disease controls. The results highlighted that anti-tTG IgA exhibited a higher sensitivity for CD (93.4%) than EmA IgA (92.8%), DGP IgG (81.8%) and DGP IgA (83.8%). The specificity of EmA IgA (99%) resulted to be higher than those of anti-tTG IgA (95.8%), DGP IgG (96.4%) and DGP IgA (92.1%). In patients with selective IgA deficiency, a condition closely related to CD, serological screening should include one of the three antibodies of IgG class, since anti-tTG, DGP and EmA have a very similar diagnostic accuracy in this clinical setting. According to age, there are two main diagnostic strategies for CD detection. In children, the revised ESPGHAN 2020 guidelines established that CD could be diagnosed in both symptomatic and asymptomatic children by high anti-tTG IgA titers (>10 times the cut-off) and EmA positivity with no need to obtain duodenal biopsy and HLA typing. In adult patients, although high tTG IgA titers (confirmed by EmA IgA positivity) correlate with villous atrophy, an intestinal biopsy is still considered mandatory for confirming CD diagnosis. Currently, a case finding approach in at-risk groups is preferred to mass screening for CD detection.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


