Bence Gunda, Ain Neuhaus, Ildikó Sipos, Rita Stang, Péter Pál Böjti, Tímea Takács, Dániel Bereczki, Balázs Kis, István Szikora, George Harston
{"title":"使用ai决策支持改善初级卒中中心的卒中护理。","authors":"Bence Gunda, Ain Neuhaus, Ildikó Sipos, Rita Stang, Péter Pál Böjti, Tímea Takács, Dániel Bereczki, Balázs Kis, István Szikora, George Harston","doi":"10.1159/000522423","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patient selection for reperfusion therapies requires significant expertise in neuroimaging. Increasingly, machine learning-based analysis is used for faster and standardized patient selection. However, there is little information on how such software influences real-world patient management.</p><p><strong>Aims: </strong>We evaluated changes in thrombolysis and thrombectomy delivery following implementation of automated analysis at a high volume primary stroke centre.</p><p><strong>Methods: </strong>We retrospectively collected data on consecutive stroke patients admitted to a large university stroke centre from two identical 7-month periods in 2017 and 2018 between which the e-Stroke Suite (Brainomix, Oxford, UK) was implemented to analyse non-contrast CT and CT angiography results. Delivery of stroke care was otherwise unchanged. Patients were transferred to a hub for thrombectomy. We collected the number of patients receiving intravenous thrombolysis and/or thrombectomy, the time to treatment; and outcome at 90 days for thrombectomy.</p><p><strong>Results: </strong>399 patients from 2017 and 398 from 2018 were included in the study. From 2017 to 2018, thrombolysis rates increased from 11.5% to 18.1% with a similar trend for thrombectomy (2.8-4.8%). There was a trend towards shorter door-to-needle times (44-42 min) and CT-to-groin puncture times (174-145 min). There was a non-significant trend towards improved outcomes with thrombectomy. Qualitatively, physician feedback suggested that e-Stroke Suite increased decision-making confidence and improved patient flow.</p><p><strong>Conclusions: </strong>Use of artificial intelligence decision support in a hyperacute stroke pathway facilitates decision-making and can improve rate and time of reperfusion therapies in a hub-and-spoke system of care.</p>","PeriodicalId":45709,"journal":{"name":"Cerebrovascular Diseases Extra","volume":"12 1","pages":"28-32"},"PeriodicalIF":2.1000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b6/db/cee-0012-0028.PMC9082202.pdf","citationCount":"1","resultStr":"{\"title\":\"Improved Stroke Care in a Primary Stroke Centre Using AI-Decision Support.\",\"authors\":\"Bence Gunda, Ain Neuhaus, Ildikó Sipos, Rita Stang, Péter Pál Böjti, Tímea Takács, Dániel Bereczki, Balázs Kis, István Szikora, George Harston\",\"doi\":\"10.1159/000522423\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Patient selection for reperfusion therapies requires significant expertise in neuroimaging. Increasingly, machine learning-based analysis is used for faster and standardized patient selection. However, there is little information on how such software influences real-world patient management.</p><p><strong>Aims: </strong>We evaluated changes in thrombolysis and thrombectomy delivery following implementation of automated analysis at a high volume primary stroke centre.</p><p><strong>Methods: </strong>We retrospectively collected data on consecutive stroke patients admitted to a large university stroke centre from two identical 7-month periods in 2017 and 2018 between which the e-Stroke Suite (Brainomix, Oxford, UK) was implemented to analyse non-contrast CT and CT angiography results. Delivery of stroke care was otherwise unchanged. Patients were transferred to a hub for thrombectomy. We collected the number of patients receiving intravenous thrombolysis and/or thrombectomy, the time to treatment; and outcome at 90 days for thrombectomy.</p><p><strong>Results: </strong>399 patients from 2017 and 398 from 2018 were included in the study. From 2017 to 2018, thrombolysis rates increased from 11.5% to 18.1% with a similar trend for thrombectomy (2.8-4.8%). There was a trend towards shorter door-to-needle times (44-42 min) and CT-to-groin puncture times (174-145 min). There was a non-significant trend towards improved outcomes with thrombectomy. Qualitatively, physician feedback suggested that e-Stroke Suite increased decision-making confidence and improved patient flow.</p><p><strong>Conclusions: </strong>Use of artificial intelligence decision support in a hyperacute stroke pathway facilitates decision-making and can improve rate and time of reperfusion therapies in a hub-and-spoke system of care.</p>\",\"PeriodicalId\":45709,\"journal\":{\"name\":\"Cerebrovascular Diseases Extra\",\"volume\":\"12 1\",\"pages\":\"28-32\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2022-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b6/db/cee-0012-0028.PMC9082202.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cerebrovascular Diseases Extra\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1159/000522423\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"PERIPHERAL VASCULAR DISEASE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cerebrovascular Diseases Extra","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000522423","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
Improved Stroke Care in a Primary Stroke Centre Using AI-Decision Support.
Background: Patient selection for reperfusion therapies requires significant expertise in neuroimaging. Increasingly, machine learning-based analysis is used for faster and standardized patient selection. However, there is little information on how such software influences real-world patient management.
Aims: We evaluated changes in thrombolysis and thrombectomy delivery following implementation of automated analysis at a high volume primary stroke centre.
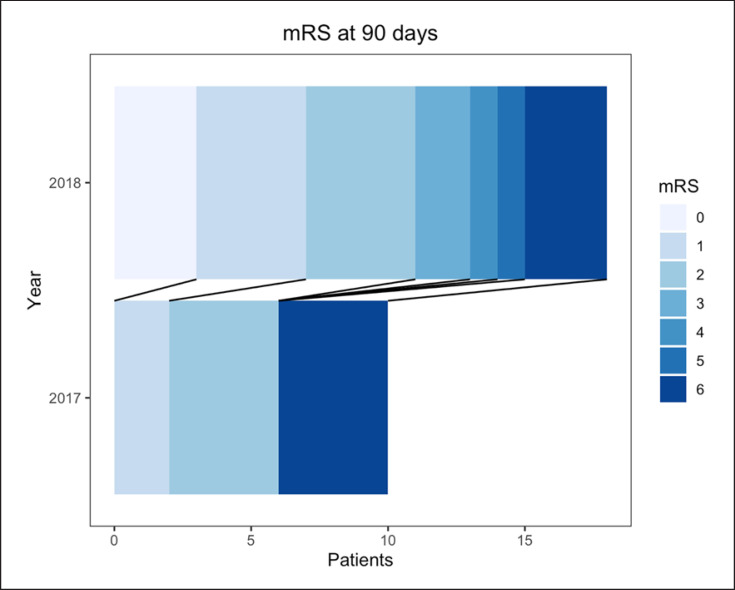
Methods: We retrospectively collected data on consecutive stroke patients admitted to a large university stroke centre from two identical 7-month periods in 2017 and 2018 between which the e-Stroke Suite (Brainomix, Oxford, UK) was implemented to analyse non-contrast CT and CT angiography results. Delivery of stroke care was otherwise unchanged. Patients were transferred to a hub for thrombectomy. We collected the number of patients receiving intravenous thrombolysis and/or thrombectomy, the time to treatment; and outcome at 90 days for thrombectomy.
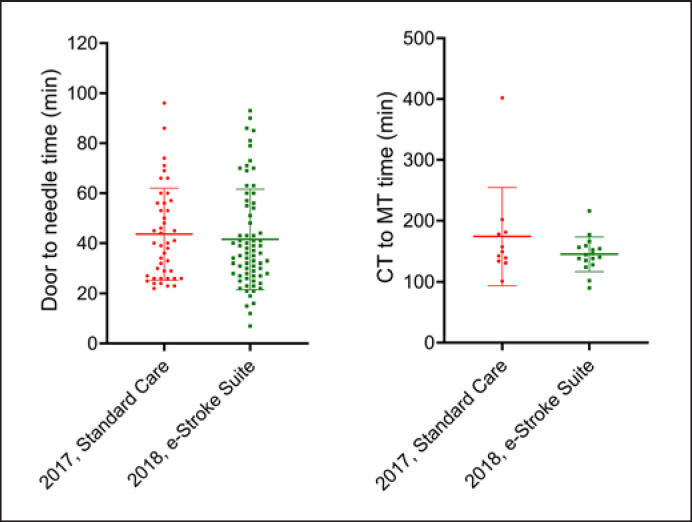
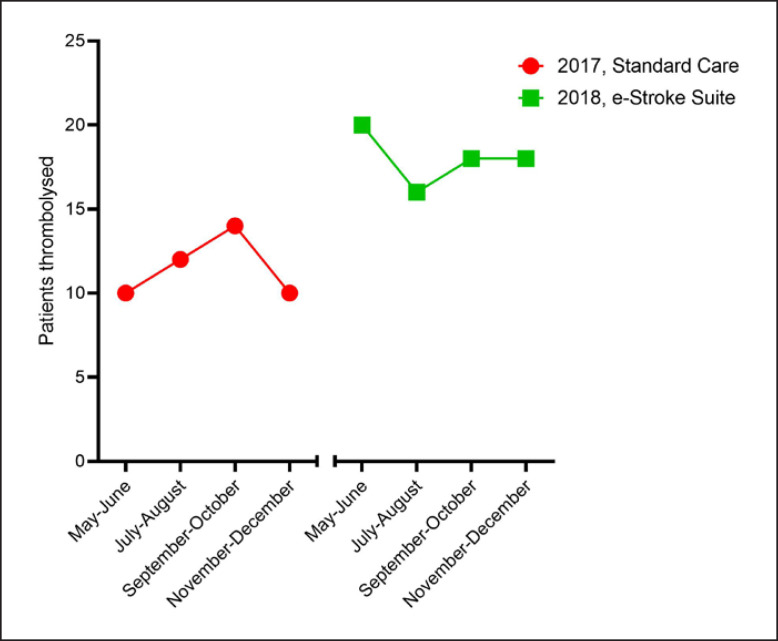
Results: 399 patients from 2017 and 398 from 2018 were included in the study. From 2017 to 2018, thrombolysis rates increased from 11.5% to 18.1% with a similar trend for thrombectomy (2.8-4.8%). There was a trend towards shorter door-to-needle times (44-42 min) and CT-to-groin puncture times (174-145 min). There was a non-significant trend towards improved outcomes with thrombectomy. Qualitatively, physician feedback suggested that e-Stroke Suite increased decision-making confidence and improved patient flow.
Conclusions: Use of artificial intelligence decision support in a hyperacute stroke pathway facilitates decision-making and can improve rate and time of reperfusion therapies in a hub-and-spoke system of care.
期刊介绍:
This open access and online-only journal publishes original articles covering the entire spectrum of stroke and cerebrovascular research, drawing from a variety of specialties such as neurology, internal medicine, surgery, radiology, epidemiology, cardiology, hematology, psychology and rehabilitation. Offering an international forum, it meets the growing need for sophisticated, up-to-date scientific information on clinical data, diagnostic testing, and therapeutic issues. The journal publishes original contributions, reviews of selected topics as well as clinical investigative studies. All aspects related to clinical advances are considered, while purely experimental work appears only if directly relevant to clinical issues. Cerebrovascular Diseases Extra provides additional contents based on reviewed and accepted submissions to the main journal Cerebrovascular Diseases.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


