{"title":"结节病的肺纤维化。","authors":"Huda Asif, Manuel Ribeiro Neto, Daniel Culver","doi":"10.36141/svdld.v40i3.14830","DOIUrl":null,"url":null,"abstract":"<p><p>Sarcoidosis may progress to pulmonary fibrosis in 5% of patients with significantly increased mortality. Histopathology shows fibrosis in a lymphangitic pattern surrounding the granulomas. Th1 to Th2 shift in environment along with angiogenesis is implicated in exuberant fibrosis. Clinical features include dyspnea, cough, and frequently with pulmonary function tests showing a mixed ventilatory defect with severely decreased diffusion capacity of carbon monoxide. Serologic markers including soluble interleukin 2 receptor, chitotriosidase and kern von den lunges 6, and chemokine ligand 18 are elevated and implicated in progression of disease. CT imaging shows fibrosis along bronchovascular bundles with reticulations, traction bronchiectasis and honeycombing predominantly in the upper and central distribution. Complications include sarcoidosis-associated pulmonary hypertension (SAPH) and chronic pulmonary aspergillosis. Treatment involves glucocorticoids and steroid-sparing agents in the presence of active granulomas. Anti-fibrotic agents such as pirfenidone and nintedanib have been shown to slow down pulmonary function decline in randomized clinical trials involving sarcoidosis-associated pulmonary fibrosis. Transplant workup is indicated in New York Heart Association class III or IV with similar success rates as in other lung transplant patients.</p>","PeriodicalId":21394,"journal":{"name":"Sarcoidosis, Vasculitis, and Diffuse Lung Diseases","volume":"40 3","pages":"e2023027"},"PeriodicalIF":1.8000,"publicationDate":"2023-09-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/2e/05/SVDLD-40-27.PMC10540713.pdf","citationCount":"0","resultStr":"{\"title\":\"Pulmonary fibrosis in sarcoidosis.\",\"authors\":\"Huda Asif, Manuel Ribeiro Neto, Daniel Culver\",\"doi\":\"10.36141/svdld.v40i3.14830\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Sarcoidosis may progress to pulmonary fibrosis in 5% of patients with significantly increased mortality. Histopathology shows fibrosis in a lymphangitic pattern surrounding the granulomas. Th1 to Th2 shift in environment along with angiogenesis is implicated in exuberant fibrosis. Clinical features include dyspnea, cough, and frequently with pulmonary function tests showing a mixed ventilatory defect with severely decreased diffusion capacity of carbon monoxide. Serologic markers including soluble interleukin 2 receptor, chitotriosidase and kern von den lunges 6, and chemokine ligand 18 are elevated and implicated in progression of disease. CT imaging shows fibrosis along bronchovascular bundles with reticulations, traction bronchiectasis and honeycombing predominantly in the upper and central distribution. Complications include sarcoidosis-associated pulmonary hypertension (SAPH) and chronic pulmonary aspergillosis. Treatment involves glucocorticoids and steroid-sparing agents in the presence of active granulomas. Anti-fibrotic agents such as pirfenidone and nintedanib have been shown to slow down pulmonary function decline in randomized clinical trials involving sarcoidosis-associated pulmonary fibrosis. Transplant workup is indicated in New York Heart Association class III or IV with similar success rates as in other lung transplant patients.</p>\",\"PeriodicalId\":21394,\"journal\":{\"name\":\"Sarcoidosis, Vasculitis, and Diffuse Lung Diseases\",\"volume\":\"40 3\",\"pages\":\"e2023027\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2023-09-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/2e/05/SVDLD-40-27.PMC10540713.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Sarcoidosis, Vasculitis, and Diffuse Lung Diseases\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.36141/svdld.v40i3.14830\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Sarcoidosis, Vasculitis, and Diffuse Lung Diseases","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.36141/svdld.v40i3.14830","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
摘要
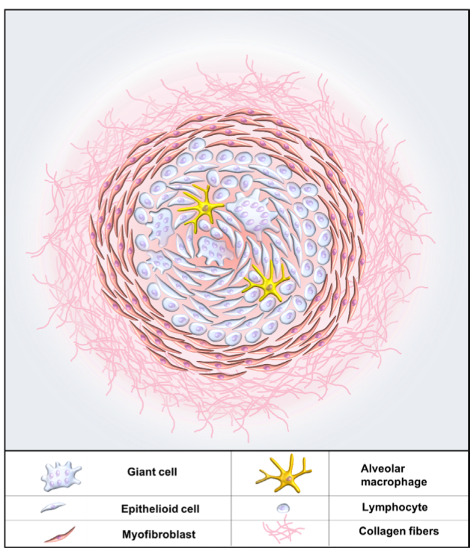
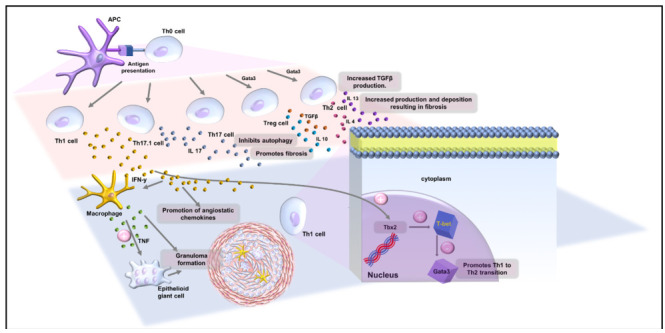
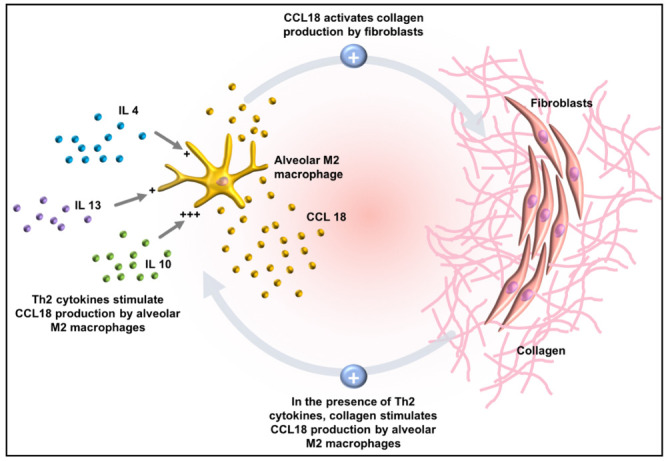
5%的患者结节病可能发展为肺纤维化,死亡率显著增加。组织病理学显示肉芽肿周围有淋巴管样纤维化。Th1至Th2在环境中的转变以及血管生成与过度纤维化有关。临床特征包括呼吸困难、咳嗽,肺功能测试显示混合通气缺陷,一氧化碳扩散能力严重降低。血清标志物,包括可溶性白细胞介素2受体、壳三糖苷酶和kern-von den rungs 6,以及趋化因子配体18升高,并与疾病进展有关。CT显示支气管血管束纤维化,网状,牵引性支气管扩张和蜂窝状,主要分布在上部和中部。并发症包括结节病相关的肺动脉高压(SAPH)和慢性肺曲霉菌病。治疗包括在存在活动性肉芽肿的情况下使用糖皮质激素和类固醇保留剂。在涉及结节病相关肺纤维化的随机临床试验中,吡非尼酮和宁替达尼等抗纤维化药物已被证明可以减缓肺功能下降。纽约心脏协会III级或IV级患者的移植检查与其他肺移植患者的成功率相似。
Sarcoidosis may progress to pulmonary fibrosis in 5% of patients with significantly increased mortality. Histopathology shows fibrosis in a lymphangitic pattern surrounding the granulomas. Th1 to Th2 shift in environment along with angiogenesis is implicated in exuberant fibrosis. Clinical features include dyspnea, cough, and frequently with pulmonary function tests showing a mixed ventilatory defect with severely decreased diffusion capacity of carbon monoxide. Serologic markers including soluble interleukin 2 receptor, chitotriosidase and kern von den lunges 6, and chemokine ligand 18 are elevated and implicated in progression of disease. CT imaging shows fibrosis along bronchovascular bundles with reticulations, traction bronchiectasis and honeycombing predominantly in the upper and central distribution. Complications include sarcoidosis-associated pulmonary hypertension (SAPH) and chronic pulmonary aspergillosis. Treatment involves glucocorticoids and steroid-sparing agents in the presence of active granulomas. Anti-fibrotic agents such as pirfenidone and nintedanib have been shown to slow down pulmonary function decline in randomized clinical trials involving sarcoidosis-associated pulmonary fibrosis. Transplant workup is indicated in New York Heart Association class III or IV with similar success rates as in other lung transplant patients.
期刊介绍:
Sarcoidosis Vasculitis and Diffuse Lung Disease is a quarterly journal founded in 1984 by G. Rizzato. Now directed by R. Baughman (Cincinnati), P. Rottoli (Siena) and S. Tomassetti (Forlì), is the oldest and most prestigious Italian journal in such field.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


