Tae Hyun Kim, Bo Hyun Kim, Yu Ri Cho, Young-Hwan Koh, Joong-Won Park
{"title":"atezolizumab联合贝伐单抗治疗晚期肝细胞癌患者额外放疗的可行性。","authors":"Tae Hyun Kim, Bo Hyun Kim, Yu Ri Cho, Young-Hwan Koh, Joong-Won Park","doi":"10.17998/jlc.2023.04.14","DOIUrl":null,"url":null,"abstract":"<p><strong>Background/aim: </strong>Radiotherapy (RT) is an effective local treatment for hepatocellular carcinoma (HCC). However, whether additional RT is safe and effective in patients with advanced HCC receiving atezolizumab plus bevacizumab remains unclear. This retrospective cohort study aimed to evaluate the feasibility of additional RT in these patients.</p><p><strong>Methods: </strong>Between March and October 2021, we retrospectively analyzed seven patients with advanced HCC who received RT during treatment with atezolizumab plus bevacizumab. The median prescribed RT dose was 35 Gy (range, 33-66). Freedom from local progression (FFLP), progression-free survival (PFS), and overall survival (OS) after RT were analyzed.</p><p><strong>Results: </strong>The median follow-up duration after RT was 14.2 months (range, 10.0-18.6). Of the seven patients, disease progression was noted in six (85.7%), the sites of disease progression were local in two (28.6%), intrahepatic in four (57.1%), and extrahepatic in four (57.1%). The median time of FFLP was not reached, and PFS and OS times were 4.0 (95% confidence interval [CI], 3.6-4.5) and 14.8% (95% CI, 12.5-17.2) months, respectively. The 1-year FFLP, PFS, and OS rates were 60% (95% CI, 43.8-76.2), 0%, and 85.7% (95% CI, 75.9-95.5), respectively. Grade 3 or higher hematologic adverse events (AEs) were not observed, but grade 3 nonhematologic AEs unrelated to RT were observed in one patient.</p><p><strong>Conclusions: </strong>The addition of RT may be feasible in patients with advanced HCC treated with atezolizumab plus bevacizumab. However, further studies are required to validate these findings.</p>","PeriodicalId":16226,"journal":{"name":"Journal of Liver Cancer","volume":" ","pages":"330-340"},"PeriodicalIF":0.0000,"publicationDate":"2023-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/97/3d/jlc-2023-04-14.PMC10565546.pdf","citationCount":"1","resultStr":"{\"title\":\"Feasibility of additional radiotherapy in patients with advanced hepatocellular carcinoma treated with atezolizumab plus bevacizumab.\",\"authors\":\"Tae Hyun Kim, Bo Hyun Kim, Yu Ri Cho, Young-Hwan Koh, Joong-Won Park\",\"doi\":\"10.17998/jlc.2023.04.14\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background/aim: </strong>Radiotherapy (RT) is an effective local treatment for hepatocellular carcinoma (HCC). However, whether additional RT is safe and effective in patients with advanced HCC receiving atezolizumab plus bevacizumab remains unclear. This retrospective cohort study aimed to evaluate the feasibility of additional RT in these patients.</p><p><strong>Methods: </strong>Between March and October 2021, we retrospectively analyzed seven patients with advanced HCC who received RT during treatment with atezolizumab plus bevacizumab. The median prescribed RT dose was 35 Gy (range, 33-66). Freedom from local progression (FFLP), progression-free survival (PFS), and overall survival (OS) after RT were analyzed.</p><p><strong>Results: </strong>The median follow-up duration after RT was 14.2 months (range, 10.0-18.6). Of the seven patients, disease progression was noted in six (85.7%), the sites of disease progression were local in two (28.6%), intrahepatic in four (57.1%), and extrahepatic in four (57.1%). The median time of FFLP was not reached, and PFS and OS times were 4.0 (95% confidence interval [CI], 3.6-4.5) and 14.8% (95% CI, 12.5-17.2) months, respectively. The 1-year FFLP, PFS, and OS rates were 60% (95% CI, 43.8-76.2), 0%, and 85.7% (95% CI, 75.9-95.5), respectively. Grade 3 or higher hematologic adverse events (AEs) were not observed, but grade 3 nonhematologic AEs unrelated to RT were observed in one patient.</p><p><strong>Conclusions: </strong>The addition of RT may be feasible in patients with advanced HCC treated with atezolizumab plus bevacizumab. However, further studies are required to validate these findings.</p>\",\"PeriodicalId\":16226,\"journal\":{\"name\":\"Journal of Liver Cancer\",\"volume\":\" \",\"pages\":\"330-340\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/97/3d/jlc-2023-04-14.PMC10565546.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Liver Cancer\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.17998/jlc.2023.04.14\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/5/16 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Liver Cancer","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.17998/jlc.2023.04.14","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/5/16 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Feasibility of additional radiotherapy in patients with advanced hepatocellular carcinoma treated with atezolizumab plus bevacizumab.
Background/aim: Radiotherapy (RT) is an effective local treatment for hepatocellular carcinoma (HCC). However, whether additional RT is safe and effective in patients with advanced HCC receiving atezolizumab plus bevacizumab remains unclear. This retrospective cohort study aimed to evaluate the feasibility of additional RT in these patients.
Methods: Between March and October 2021, we retrospectively analyzed seven patients with advanced HCC who received RT during treatment with atezolizumab plus bevacizumab. The median prescribed RT dose was 35 Gy (range, 33-66). Freedom from local progression (FFLP), progression-free survival (PFS), and overall survival (OS) after RT were analyzed.
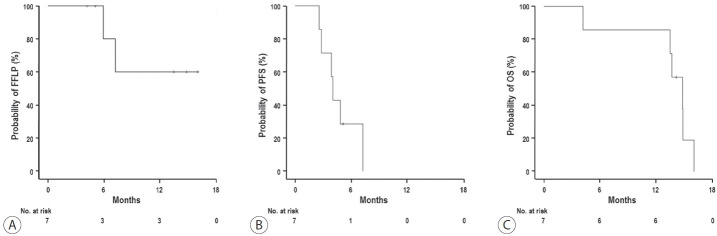
Results: The median follow-up duration after RT was 14.2 months (range, 10.0-18.6). Of the seven patients, disease progression was noted in six (85.7%), the sites of disease progression were local in two (28.6%), intrahepatic in four (57.1%), and extrahepatic in four (57.1%). The median time of FFLP was not reached, and PFS and OS times were 4.0 (95% confidence interval [CI], 3.6-4.5) and 14.8% (95% CI, 12.5-17.2) months, respectively. The 1-year FFLP, PFS, and OS rates were 60% (95% CI, 43.8-76.2), 0%, and 85.7% (95% CI, 75.9-95.5), respectively. Grade 3 or higher hematologic adverse events (AEs) were not observed, but grade 3 nonhematologic AEs unrelated to RT were observed in one patient.
Conclusions: The addition of RT may be feasible in patients with advanced HCC treated with atezolizumab plus bevacizumab. However, further studies are required to validate these findings.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


