Imke Redeker, Stefan Moustakis, Styliani Tsiami, Xenofon Baraliakos, Ioana Andreica, Bjoern Buehring, Jürgen Braun, Uta Kiltz
{"title":"慢性炎症性风湿病患者的阿达木单抗治疗:常规护理中患者水平治疗轨迹的研究","authors":"Imke Redeker, Stefan Moustakis, Styliani Tsiami, Xenofon Baraliakos, Ioana Andreica, Bjoern Buehring, Jürgen Braun, Uta Kiltz","doi":"10.1177/1759720X231197087","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Previous experiences with non-medical switching of adalimumab (ADA) in patients with chronic inflammatory rheumatic diseases (CIRD) come mainly from phase III extension of randomised clinical trials and little from routine care.</p><p><strong>Objectives: </strong>To analyse treatment trajectories over 2 years in patients with CIRD conducting a non-medical switch from originator to biosimilar ADA.</p><p><strong>Design: </strong>A retrospective observational cohort study was conducted with data from a third-level rheumatology centre in Germany. CIRD patients on originator ADA who switched to ADA biosimilar from October 2018 onwards were identified and followed until September 2020.</p><p><strong>Methods: </strong>Patients' characteristics were compared between the four <i>a priori</i> defined treatment trajectories 'continued biosimilar ADA therapy', 'back-switch to originator ADA therapy', 'switch to another biological disease-modifying anti-rheumatic drug (bDMARD) therapy' and 'stopped bDMARD therapy/death/drop out'. Factors associated with continuing biosimilar ADA therapy were analysed using Cox proportional hazards regression analyses.</p><p><strong>Results: </strong>A total of 121 CIRD patients were included. Most patients (66.9%) continued therapy with biosimilar ADA over 2 years, with a treatment retention rate of 73.1%. Whereas 21 patients (17.4%) switched back to originator ADA, mainly due to adverse events, and 8 patients (6.6%) switched to a different bDMARD, mainly due to lack of effect. The estimated risk of withdrawal was lower for longer prior duration on originator ADA [hazard ratio (HR): 0.82; 95% CI: 0.69-0.97] and higher for higher C-reactive protein levels at baseline (HR: 1.18; 95% CI: 1.00-1.39). Male patients, older patients and those for whom originator ADA was their first bDMARD tended to have a lower risk of withdrawal.</p><p><strong>Conclusion: </strong>Our results indicated that three of four patients continue biosimilar ADA over 2 years with lower risks of withdrawal for male sex, older age, longer prior duration on originator ADA and originator ADA as first bDMARD.</p>","PeriodicalId":23056,"journal":{"name":"Therapeutic Advances in Musculoskeletal Disease","volume":"15 ","pages":"1759720X231197087"},"PeriodicalIF":3.4000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ac/da/10.1177_1759720X231197087.PMC10492472.pdf","citationCount":"0","resultStr":"{\"title\":\"Treatment with adalimumab in patients with chronic inflammatory rheumatic diseases: a study of treatment trajectories on a patient level in routine care.\",\"authors\":\"Imke Redeker, Stefan Moustakis, Styliani Tsiami, Xenofon Baraliakos, Ioana Andreica, Bjoern Buehring, Jürgen Braun, Uta Kiltz\",\"doi\":\"10.1177/1759720X231197087\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Previous experiences with non-medical switching of adalimumab (ADA) in patients with chronic inflammatory rheumatic diseases (CIRD) come mainly from phase III extension of randomised clinical trials and little from routine care.</p><p><strong>Objectives: </strong>To analyse treatment trajectories over 2 years in patients with CIRD conducting a non-medical switch from originator to biosimilar ADA.</p><p><strong>Design: </strong>A retrospective observational cohort study was conducted with data from a third-level rheumatology centre in Germany. CIRD patients on originator ADA who switched to ADA biosimilar from October 2018 onwards were identified and followed until September 2020.</p><p><strong>Methods: </strong>Patients' characteristics were compared between the four <i>a priori</i> defined treatment trajectories 'continued biosimilar ADA therapy', 'back-switch to originator ADA therapy', 'switch to another biological disease-modifying anti-rheumatic drug (bDMARD) therapy' and 'stopped bDMARD therapy/death/drop out'. Factors associated with continuing biosimilar ADA therapy were analysed using Cox proportional hazards regression analyses.</p><p><strong>Results: </strong>A total of 121 CIRD patients were included. Most patients (66.9%) continued therapy with biosimilar ADA over 2 years, with a treatment retention rate of 73.1%. Whereas 21 patients (17.4%) switched back to originator ADA, mainly due to adverse events, and 8 patients (6.6%) switched to a different bDMARD, mainly due to lack of effect. The estimated risk of withdrawal was lower for longer prior duration on originator ADA [hazard ratio (HR): 0.82; 95% CI: 0.69-0.97] and higher for higher C-reactive protein levels at baseline (HR: 1.18; 95% CI: 1.00-1.39). Male patients, older patients and those for whom originator ADA was their first bDMARD tended to have a lower risk of withdrawal.</p><p><strong>Conclusion: </strong>Our results indicated that three of four patients continue biosimilar ADA over 2 years with lower risks of withdrawal for male sex, older age, longer prior duration on originator ADA and originator ADA as first bDMARD.</p>\",\"PeriodicalId\":23056,\"journal\":{\"name\":\"Therapeutic Advances in Musculoskeletal Disease\",\"volume\":\"15 \",\"pages\":\"1759720X231197087\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ac/da/10.1177_1759720X231197087.PMC10492472.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Therapeutic Advances in Musculoskeletal Disease\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/1759720X231197087\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"RHEUMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Musculoskeletal Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/1759720X231197087","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
Treatment with adalimumab in patients with chronic inflammatory rheumatic diseases: a study of treatment trajectories on a patient level in routine care.
Background: Previous experiences with non-medical switching of adalimumab (ADA) in patients with chronic inflammatory rheumatic diseases (CIRD) come mainly from phase III extension of randomised clinical trials and little from routine care.
Objectives: To analyse treatment trajectories over 2 years in patients with CIRD conducting a non-medical switch from originator to biosimilar ADA.
Design: A retrospective observational cohort study was conducted with data from a third-level rheumatology centre in Germany. CIRD patients on originator ADA who switched to ADA biosimilar from October 2018 onwards were identified and followed until September 2020.
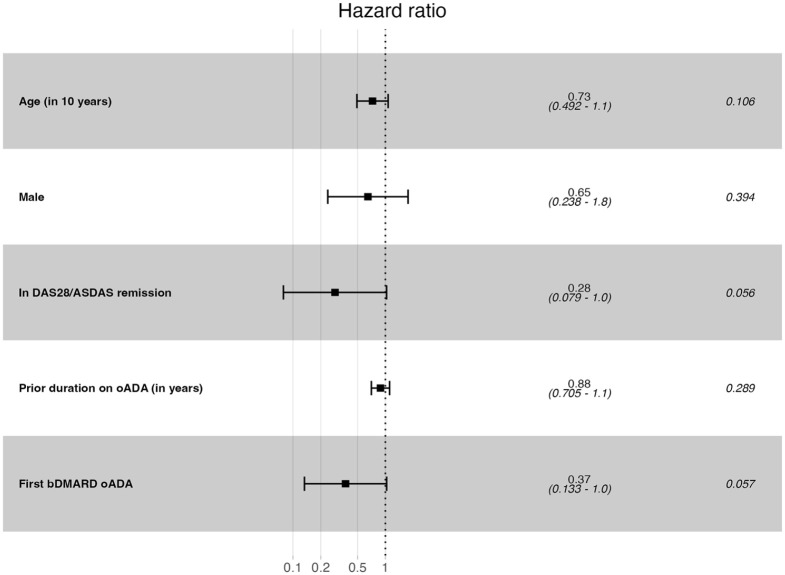
Methods: Patients' characteristics were compared between the four a priori defined treatment trajectories 'continued biosimilar ADA therapy', 'back-switch to originator ADA therapy', 'switch to another biological disease-modifying anti-rheumatic drug (bDMARD) therapy' and 'stopped bDMARD therapy/death/drop out'. Factors associated with continuing biosimilar ADA therapy were analysed using Cox proportional hazards regression analyses.
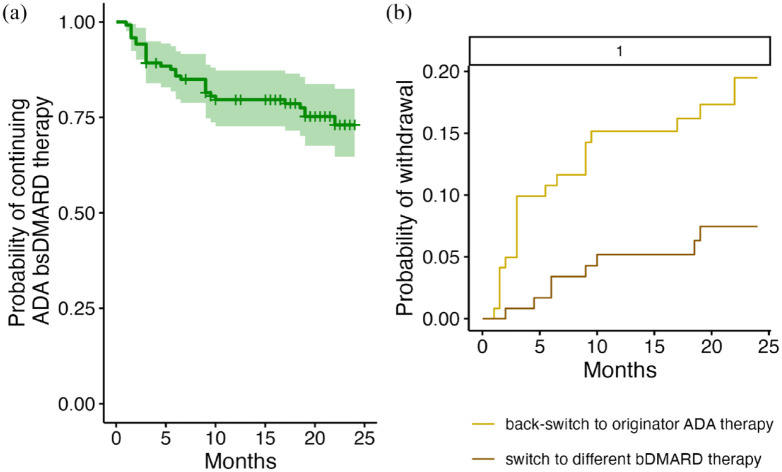
Results: A total of 121 CIRD patients were included. Most patients (66.9%) continued therapy with biosimilar ADA over 2 years, with a treatment retention rate of 73.1%. Whereas 21 patients (17.4%) switched back to originator ADA, mainly due to adverse events, and 8 patients (6.6%) switched to a different bDMARD, mainly due to lack of effect. The estimated risk of withdrawal was lower for longer prior duration on originator ADA [hazard ratio (HR): 0.82; 95% CI: 0.69-0.97] and higher for higher C-reactive protein levels at baseline (HR: 1.18; 95% CI: 1.00-1.39). Male patients, older patients and those for whom originator ADA was their first bDMARD tended to have a lower risk of withdrawal.
Conclusion: Our results indicated that three of four patients continue biosimilar ADA over 2 years with lower risks of withdrawal for male sex, older age, longer prior duration on originator ADA and originator ADA as first bDMARD.
期刊介绍:
Therapeutic Advances in Musculoskeletal Disease delivers the highest quality peer-reviewed articles, reviews, and scholarly comment on pioneering efforts and innovative studies across all areas of musculoskeletal disease.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


