{"title":"都柏林2010-2022年社区获得性尿路致病性大肠杆菌的药敏模式","authors":"Saied Ali, Laura Ryan","doi":"10.1099/acmi.0.000633.v3","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong><i>Escherichia coli</i> is a common cause of urinary tract infections. Due to the increase in antimicrobial resistance (AMR) and global differences in antimicrobial susceptibility data, routine assessment of local antimicrobial susceptibility patterns is necessary to guide the selection of appropriate empirical therapy. The aim of this study was to evaluate the antimicrobial susceptibility patterns of community-acquired uropathogenic <i>Escherichia coli</i> within a catchment area in Dublin over a 13 year period, 2010-2022.</p><p><strong>Methods: </strong>All mid-stream urine samples received from local general practitioners in which there was significant <i>E. coli</i> bacteriuria during the study period, 2010-2022, were included in the analysis. Antimicrobial susceptibility testing was performed by disc diffusion as per the European Committee on Antimicrobial Susceptibility Testing recommendations.</p><p><strong>Results: </strong>An average of 11 407 urine samples per month had significant bacteriuria, with <i>E. coli</i> accounting for an average of 67 % of those. Overall AMR rates were highest for ampicillin (53.9 %), followed by trimethoprim (32.4 %), gentamicin (18.6 %), co-amoxiclav (16.5 %), ciprofloxacin (12.3 %), cephalexin (8.3 %), cefpodoxime (6.8 %) and nitrofurantoin (2 %). While rates appeared grossly static, statistically significant reduced resistance rates were noted for co-amoxiclav (r<sub>s</sub>=-0.95; <i>P</i>=<0.001), cephalexin prior to 2019 (r<sub>s</sub>=-0.783; <i>P</i>=0.013) and trimethoprim (r<sub>s</sub>=-0.639; <i>P</i>=0.019), with a statistically significant increase in non-susceptibility to cefpodoxime (r<sub>s</sub>=0.802; <i>P</i>=0.001).</p><p><strong>Conclusions: </strong>In order to generate efficient empirical antimicrobial prescribing guidelines, knowledge of region-specific contemporaneous antimicrobial susceptibility patterns is pivotal. Our findings support the use of nitrofurantoin or cephalexin as empirical antimicrobial therapy within our setting.</p>","PeriodicalId":6956,"journal":{"name":"Access Microbiology","volume":"5 8","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10484315/pdf/","citationCount":"0","resultStr":"{\"title\":\"Antimicrobial susceptibility patterns of community-acquired uropathogenic <i>Escherichia coli</i>, Dublin 2010-2022.\",\"authors\":\"Saied Ali, Laura Ryan\",\"doi\":\"10.1099/acmi.0.000633.v3\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong><i>Escherichia coli</i> is a common cause of urinary tract infections. Due to the increase in antimicrobial resistance (AMR) and global differences in antimicrobial susceptibility data, routine assessment of local antimicrobial susceptibility patterns is necessary to guide the selection of appropriate empirical therapy. The aim of this study was to evaluate the antimicrobial susceptibility patterns of community-acquired uropathogenic <i>Escherichia coli</i> within a catchment area in Dublin over a 13 year period, 2010-2022.</p><p><strong>Methods: </strong>All mid-stream urine samples received from local general practitioners in which there was significant <i>E. coli</i> bacteriuria during the study period, 2010-2022, were included in the analysis. Antimicrobial susceptibility testing was performed by disc diffusion as per the European Committee on Antimicrobial Susceptibility Testing recommendations.</p><p><strong>Results: </strong>An average of 11 407 urine samples per month had significant bacteriuria, with <i>E. coli</i> accounting for an average of 67 % of those. Overall AMR rates were highest for ampicillin (53.9 %), followed by trimethoprim (32.4 %), gentamicin (18.6 %), co-amoxiclav (16.5 %), ciprofloxacin (12.3 %), cephalexin (8.3 %), cefpodoxime (6.8 %) and nitrofurantoin (2 %). While rates appeared grossly static, statistically significant reduced resistance rates were noted for co-amoxiclav (r<sub>s</sub>=-0.95; <i>P</i>=<0.001), cephalexin prior to 2019 (r<sub>s</sub>=-0.783; <i>P</i>=0.013) and trimethoprim (r<sub>s</sub>=-0.639; <i>P</i>=0.019), with a statistically significant increase in non-susceptibility to cefpodoxime (r<sub>s</sub>=0.802; <i>P</i>=0.001).</p><p><strong>Conclusions: </strong>In order to generate efficient empirical antimicrobial prescribing guidelines, knowledge of region-specific contemporaneous antimicrobial susceptibility patterns is pivotal. Our findings support the use of nitrofurantoin or cephalexin as empirical antimicrobial therapy within our setting.</p>\",\"PeriodicalId\":6956,\"journal\":{\"name\":\"Access Microbiology\",\"volume\":\"5 8\",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10484315/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Access Microbiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1099/acmi.0.000633.v3\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Access Microbiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1099/acmi.0.000633.v3","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:大肠杆菌是尿路感染的常见原因。由于抗菌素耐药性(AMR)的增加和全球抗菌素敏感性数据的差异,有必要对当地抗菌素敏感性模式进行常规评估,以指导选择适当的经验治疗。本研究的目的是评估2010年至2022年13年间都柏林一个集水区社区获得性尿路致病性大肠杆菌的抗菌药物敏感性模式。方法:选取2010-2022年研究期间所有从当地全科医生处采集的有明显大肠杆菌尿的中游尿液样本进行分析。根据欧洲抗微生物药敏试验委员会的建议,采用圆盘扩散法进行抗微生物药敏试验。结果:每月平均11 407份尿样有明显的细菌尿,其中大肠杆菌平均占67%。氨苄西林总体AMR率最高(53.9%),其次是甲氧苄啶(32.4%)、庆大霉素(18.6%)、复方阿莫昔酸(16.5%)、环丙沙星(12.3%)、头孢氨苄(8.3%)、头孢多肟(6.8%)和呋喃妥因(2%)。虽然耐药率基本保持不变,但在统计学上显著降低了共阿莫昔拉夫的耐药率(rs=-0.95;P = s = -0.783;P=0.013)和甲氧苄啶(rs=-0.639;P=0.019),对头孢多肟不敏感的患者增加有统计学意义(rs=0.802;P = 0.001)。结论:为了制定有效的经验性抗菌药物处方指南,了解区域特异性同期抗菌药物敏感性模式至关重要。我们的研究结果支持在我们的环境中使用呋喃妥因或头孢氨苄作为经验性抗菌治疗。
Antimicrobial susceptibility patterns of community-acquired uropathogenic Escherichia coli, Dublin 2010-2022.
Background: Escherichia coli is a common cause of urinary tract infections. Due to the increase in antimicrobial resistance (AMR) and global differences in antimicrobial susceptibility data, routine assessment of local antimicrobial susceptibility patterns is necessary to guide the selection of appropriate empirical therapy. The aim of this study was to evaluate the antimicrobial susceptibility patterns of community-acquired uropathogenic Escherichia coli within a catchment area in Dublin over a 13 year period, 2010-2022.
Methods: All mid-stream urine samples received from local general practitioners in which there was significant E. coli bacteriuria during the study period, 2010-2022, were included in the analysis. Antimicrobial susceptibility testing was performed by disc diffusion as per the European Committee on Antimicrobial Susceptibility Testing recommendations.
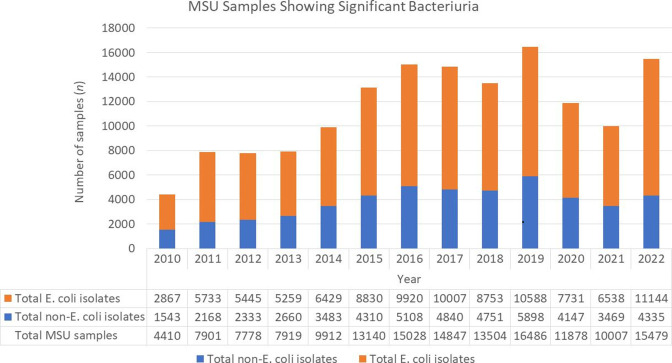
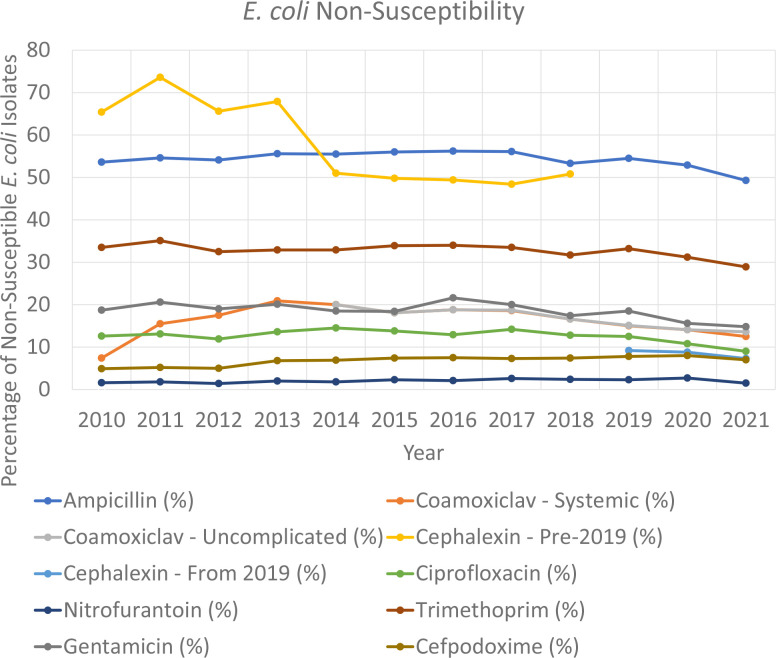
Results: An average of 11 407 urine samples per month had significant bacteriuria, with E. coli accounting for an average of 67 % of those. Overall AMR rates were highest for ampicillin (53.9 %), followed by trimethoprim (32.4 %), gentamicin (18.6 %), co-amoxiclav (16.5 %), ciprofloxacin (12.3 %), cephalexin (8.3 %), cefpodoxime (6.8 %) and nitrofurantoin (2 %). While rates appeared grossly static, statistically significant reduced resistance rates were noted for co-amoxiclav (rs=-0.95; P=<0.001), cephalexin prior to 2019 (rs=-0.783; P=0.013) and trimethoprim (rs=-0.639; P=0.019), with a statistically significant increase in non-susceptibility to cefpodoxime (rs=0.802; P=0.001).
Conclusions: In order to generate efficient empirical antimicrobial prescribing guidelines, knowledge of region-specific contemporaneous antimicrobial susceptibility patterns is pivotal. Our findings support the use of nitrofurantoin or cephalexin as empirical antimicrobial therapy within our setting.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


