Joon Young Kim, Won Chul Cho, Dong-Hee Kim, Eun Seok Choi, Bo Sang Kwon, Tae-Jin Yun, Chun Soo Park
{"title":"先天性心脏病患儿机械主动脉瓣置换术后的疗效。","authors":"Joon Young Kim, Won Chul Cho, Dong-Hee Kim, Eun Seok Choi, Bo Sang Kwon, Tae-Jin Yun, Chun Soo Park","doi":"10.5090/jcs.23.071","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The optimal choice of valve substitute for aortic valve replacement (AVR) in pediatric patients remains a matter of debate. This study investigated the outcomes following AVR using mechanical prostheses in children.</p><p><strong>Methods: </strong>Forty-four patients younger than 15 years who underwent mechanical AVR from March 1990 through March 2023 were included. The outcomes of interest were death or transplantation, hemorrhagic or thromboembolic events, and reoperation after mechanical AVR. Adverse events included any death, transplant, aortic valve reoperation, and major thromboembolic or hemorrhagic event.</p><p><strong>Results: </strong>The median age and weight at AVR were 139 months and 32 kg, respectively. The median follow-up duration was 56 months. The most commonly used valve size was 21 mm (14 [31.8%]). There were 2 in-hospital deaths, 1 in-hospital transplant, and 1 late death. The overall survival rates at 1 and 10 years post-AVR were 92.9% and 90.0%, respectively. Aortic valve reoperation was required in 4 patients at a median of 70 months post-AVR. No major hemorrhagic or thromboembolic events occurred. The 5- and 10-year adverse event-free survival rates were 81.8% and 72.2%, respectively. In univariable analysis, younger age, longer cardiopulmonary bypass time, and smaller valve size were associated with adverse events. The cut-off values for age and prosthetic valve size to minimize the risk of adverse events were 71 months and 20 mm, respectively.</p><p><strong>Conclusion: </strong>Mechanical AVR could be performed safely in children. Younger age, longer cardiopulmonary bypass time and smaller valve size were associated with adverse events. Thromboembolic or hemorrhagic complications might rarely occur.</p>","PeriodicalId":34499,"journal":{"name":"Journal of Chest Surgery","volume":" ","pages":"394-402"},"PeriodicalIF":0.0000,"publicationDate":"2023-11-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10625956/pdf/","citationCount":"0","resultStr":"{\"title\":\"Outcomes after Mechanical Aortic Valve Replacement in Children with Congenital Heart Disease.\",\"authors\":\"Joon Young Kim, Won Chul Cho, Dong-Hee Kim, Eun Seok Choi, Bo Sang Kwon, Tae-Jin Yun, Chun Soo Park\",\"doi\":\"10.5090/jcs.23.071\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The optimal choice of valve substitute for aortic valve replacement (AVR) in pediatric patients remains a matter of debate. This study investigated the outcomes following AVR using mechanical prostheses in children.</p><p><strong>Methods: </strong>Forty-four patients younger than 15 years who underwent mechanical AVR from March 1990 through March 2023 were included. The outcomes of interest were death or transplantation, hemorrhagic or thromboembolic events, and reoperation after mechanical AVR. Adverse events included any death, transplant, aortic valve reoperation, and major thromboembolic or hemorrhagic event.</p><p><strong>Results: </strong>The median age and weight at AVR were 139 months and 32 kg, respectively. The median follow-up duration was 56 months. The most commonly used valve size was 21 mm (14 [31.8%]). There were 2 in-hospital deaths, 1 in-hospital transplant, and 1 late death. The overall survival rates at 1 and 10 years post-AVR were 92.9% and 90.0%, respectively. Aortic valve reoperation was required in 4 patients at a median of 70 months post-AVR. No major hemorrhagic or thromboembolic events occurred. The 5- and 10-year adverse event-free survival rates were 81.8% and 72.2%, respectively. In univariable analysis, younger age, longer cardiopulmonary bypass time, and smaller valve size were associated with adverse events. The cut-off values for age and prosthetic valve size to minimize the risk of adverse events were 71 months and 20 mm, respectively.</p><p><strong>Conclusion: </strong>Mechanical AVR could be performed safely in children. Younger age, longer cardiopulmonary bypass time and smaller valve size were associated with adverse events. Thromboembolic or hemorrhagic complications might rarely occur.</p>\",\"PeriodicalId\":34499,\"journal\":{\"name\":\"Journal of Chest Surgery\",\"volume\":\" \",\"pages\":\"394-402\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-11-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10625956/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Chest Surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5090/jcs.23.071\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/9/12 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Chest Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5090/jcs.23.071","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/9/12 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
Outcomes after Mechanical Aortic Valve Replacement in Children with Congenital Heart Disease.
Background: The optimal choice of valve substitute for aortic valve replacement (AVR) in pediatric patients remains a matter of debate. This study investigated the outcomes following AVR using mechanical prostheses in children.
Methods: Forty-four patients younger than 15 years who underwent mechanical AVR from March 1990 through March 2023 were included. The outcomes of interest were death or transplantation, hemorrhagic or thromboembolic events, and reoperation after mechanical AVR. Adverse events included any death, transplant, aortic valve reoperation, and major thromboembolic or hemorrhagic event.
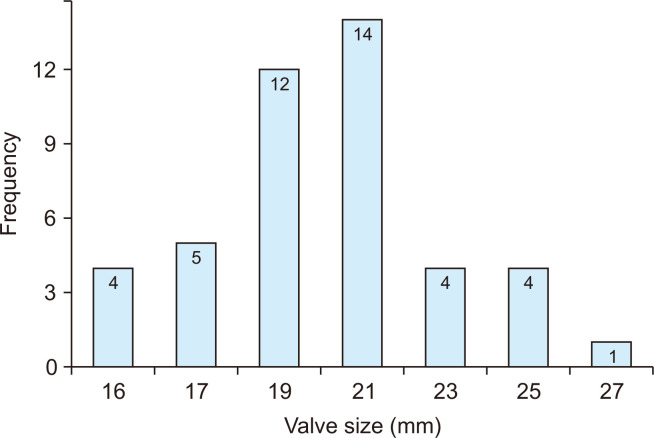
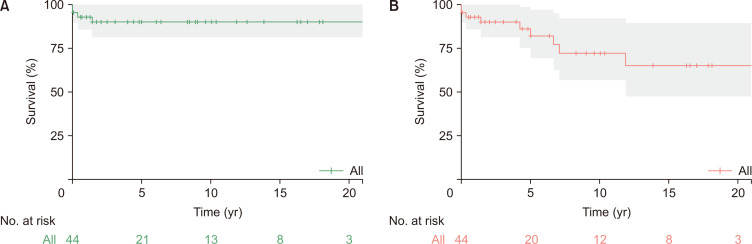
Results: The median age and weight at AVR were 139 months and 32 kg, respectively. The median follow-up duration was 56 months. The most commonly used valve size was 21 mm (14 [31.8%]). There were 2 in-hospital deaths, 1 in-hospital transplant, and 1 late death. The overall survival rates at 1 and 10 years post-AVR were 92.9% and 90.0%, respectively. Aortic valve reoperation was required in 4 patients at a median of 70 months post-AVR. No major hemorrhagic or thromboembolic events occurred. The 5- and 10-year adverse event-free survival rates were 81.8% and 72.2%, respectively. In univariable analysis, younger age, longer cardiopulmonary bypass time, and smaller valve size were associated with adverse events. The cut-off values for age and prosthetic valve size to minimize the risk of adverse events were 71 months and 20 mm, respectively.
Conclusion: Mechanical AVR could be performed safely in children. Younger age, longer cardiopulmonary bypass time and smaller valve size were associated with adverse events. Thromboembolic or hemorrhagic complications might rarely occur.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


