Nancy K Glober, Tyler Fulks, Michael Supples, Peter Panagos, David Kim
{"title":"预测医务人员对急性缺血性卒中和大血管闭塞的误诊的因素。","authors":"Nancy K Glober, Tyler Fulks, Michael Supples, Peter Panagos, David Kim","doi":"10.1097/HPC.0000000000000307","DOIUrl":null,"url":null,"abstract":"<p><p>The emergence of thrombectomy for large vessel occlusions has increased the importance of accurate prehospital identification and triage of acute ischemic stroke (AIS). Despite available clinical scores, prehospital identification is suboptimal. Our objective was to improve the sensitivity of prehospital AIS identification by combining dispatch information with paramedic impression. We performed a retrospective cohort review of emergency medical services and hospital records of all patients for whom a stroke alert was activated in 1 urban, academic emergency department from January 1, 2018, to December 31, 2019. Using admission diagnosis of acute stroke as outcome, we calculated the sensitivity and specificity of dispatch and paramedic impression in identifying AIS and large vessel occlusion. We identified factors that, when included together, would improve the sensitivity of prehospital AIS identification. Two-hundred twenty-six stroke alerts were activated by emergency department physicians after transport by Indianapolis emergency medical services. Forty-four percent (99/226) were female, median age was 58 years (interquartile range, 50-67 years), and median National Institutes of Health Stroke Scale was 6 (interquartile range, 2-12). Paramedics demonstrated superior sensitivity (59% vs. 48%) but inferior specificity (56% vs. 73%) for detection of stroke as compared with dispatch. A strategy incorporating dispatch code of stroke, or paramedic impression of altered mental status or weakness in addition to stroke, would be 84% sensitive and 27% specific for identification of stroke. To optimize rapid and sensitive stroke detection, prehospital systems should consider inclusion of patients with dispatch code of stroke and provider impression of altered mental status or generalized weakness.</p>","PeriodicalId":35914,"journal":{"name":"Critical Pathways in Cardiology","volume":"21 4","pages":"172-175"},"PeriodicalIF":0.0000,"publicationDate":"2022-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/4a/42/hpc-21-172.PMC9678438.pdf","citationCount":"0","resultStr":"{\"title\":\"Factors Predicting Misidentification of Acute Ischemic Stroke and Large Vessel Occlusion by Paramedics.\",\"authors\":\"Nancy K Glober, Tyler Fulks, Michael Supples, Peter Panagos, David Kim\",\"doi\":\"10.1097/HPC.0000000000000307\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The emergence of thrombectomy for large vessel occlusions has increased the importance of accurate prehospital identification and triage of acute ischemic stroke (AIS). Despite available clinical scores, prehospital identification is suboptimal. Our objective was to improve the sensitivity of prehospital AIS identification by combining dispatch information with paramedic impression. We performed a retrospective cohort review of emergency medical services and hospital records of all patients for whom a stroke alert was activated in 1 urban, academic emergency department from January 1, 2018, to December 31, 2019. Using admission diagnosis of acute stroke as outcome, we calculated the sensitivity and specificity of dispatch and paramedic impression in identifying AIS and large vessel occlusion. We identified factors that, when included together, would improve the sensitivity of prehospital AIS identification. Two-hundred twenty-six stroke alerts were activated by emergency department physicians after transport by Indianapolis emergency medical services. Forty-four percent (99/226) were female, median age was 58 years (interquartile range, 50-67 years), and median National Institutes of Health Stroke Scale was 6 (interquartile range, 2-12). Paramedics demonstrated superior sensitivity (59% vs. 48%) but inferior specificity (56% vs. 73%) for detection of stroke as compared with dispatch. A strategy incorporating dispatch code of stroke, or paramedic impression of altered mental status or weakness in addition to stroke, would be 84% sensitive and 27% specific for identification of stroke. To optimize rapid and sensitive stroke detection, prehospital systems should consider inclusion of patients with dispatch code of stroke and provider impression of altered mental status or generalized weakness.</p>\",\"PeriodicalId\":35914,\"journal\":{\"name\":\"Critical Pathways in Cardiology\",\"volume\":\"21 4\",\"pages\":\"172-175\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/4a/42/hpc-21-172.PMC9678438.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical Pathways in Cardiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/HPC.0000000000000307\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Pathways in Cardiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/HPC.0000000000000307","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
Factors Predicting Misidentification of Acute Ischemic Stroke and Large Vessel Occlusion by Paramedics.
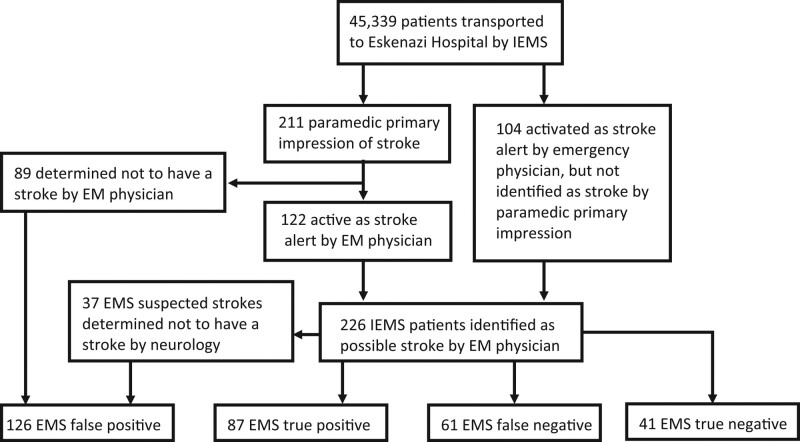
The emergence of thrombectomy for large vessel occlusions has increased the importance of accurate prehospital identification and triage of acute ischemic stroke (AIS). Despite available clinical scores, prehospital identification is suboptimal. Our objective was to improve the sensitivity of prehospital AIS identification by combining dispatch information with paramedic impression. We performed a retrospective cohort review of emergency medical services and hospital records of all patients for whom a stroke alert was activated in 1 urban, academic emergency department from January 1, 2018, to December 31, 2019. Using admission diagnosis of acute stroke as outcome, we calculated the sensitivity and specificity of dispatch and paramedic impression in identifying AIS and large vessel occlusion. We identified factors that, when included together, would improve the sensitivity of prehospital AIS identification. Two-hundred twenty-six stroke alerts were activated by emergency department physicians after transport by Indianapolis emergency medical services. Forty-four percent (99/226) were female, median age was 58 years (interquartile range, 50-67 years), and median National Institutes of Health Stroke Scale was 6 (interquartile range, 2-12). Paramedics demonstrated superior sensitivity (59% vs. 48%) but inferior specificity (56% vs. 73%) for detection of stroke as compared with dispatch. A strategy incorporating dispatch code of stroke, or paramedic impression of altered mental status or weakness in addition to stroke, would be 84% sensitive and 27% specific for identification of stroke. To optimize rapid and sensitive stroke detection, prehospital systems should consider inclusion of patients with dispatch code of stroke and provider impression of altered mental status or generalized weakness.
期刊介绍:
Critical Pathways in Cardiology provides a single source for the diagnostic and therapeutic protocols in use at hospitals worldwide for patients with cardiac disorders. The Journal presents critical pathways for specific diagnoses—complete with evidence-based rationales—and also publishes studies of these protocols" effectiveness.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


