Amy L King, Courtney M Brown, Cynthia C White, Kristen A Copeland
{"title":"利用质量改进设计初级保健幼儿服务导航。","authors":"Amy L King, Courtney M Brown, Cynthia C White, Kristen A Copeland","doi":"10.1097/pq9.0000000000000662","DOIUrl":null,"url":null,"abstract":"<p><p>Enrollment in high-quality early childhood education (ECE) improves educational and health outcomes and can mitigate racial and economic disparities. Pediatricians are encouraged to promote ECE yet lack the time and knowledge to assist families effectively. In 2016, our academic primary care center hired an ECE Navigator to promote ECE and help families enroll. Our SMART aims were to increase the number of children with facilitated referrals to high-quality ECE programs from 0 to 15 per month and to confirm enrollment on a subset to achieve an enrollment rate of 50% by December 31, 2020.</p><p><strong>Methods: </strong>We used the Institute for Healthcare Improvement's Model for Improvement. Interventions included system changes in partnership with ECE agencies (eg, interactive map of subsidized preschool options, streamlined enrollment forms), case management with families, and population-based approaches to understand families' needs and the program's overall impact. We plotted the number of monthly facilitated referrals and the percentage of referrals enrolled on run and control charts. We used standard probability-based rules to identify special causes.</p><p><strong>Results: </strong>Facilitated referrals increased from 0 to 29 per month and remained above 15. The percentage of enrolled referrals increased from 30% to 74% in 2018, then decreased to 27% in 2020 when childcare availability declined during the pandemic.</p><p><strong>Conclusions: </strong>Our innovative ECE partnership improved access to high-quality ECE. Interventions could be adopted in part or whole by other clinical practices or WIC offices to equitably improve early childhood experiences for low-income families and racial minorities.</p>","PeriodicalId":74412,"journal":{"name":"Pediatric quality & safety","volume":null,"pages":null},"PeriodicalIF":1.2000,"publicationDate":"2023-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/57/c4/pqs-8-e662.PMC10332832.pdf","citationCount":"0","resultStr":"{\"title\":\"Using Quality Improvement to Design Early Childhood Services Navigation in Primary Care.\",\"authors\":\"Amy L King, Courtney M Brown, Cynthia C White, Kristen A Copeland\",\"doi\":\"10.1097/pq9.0000000000000662\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Enrollment in high-quality early childhood education (ECE) improves educational and health outcomes and can mitigate racial and economic disparities. Pediatricians are encouraged to promote ECE yet lack the time and knowledge to assist families effectively. In 2016, our academic primary care center hired an ECE Navigator to promote ECE and help families enroll. Our SMART aims were to increase the number of children with facilitated referrals to high-quality ECE programs from 0 to 15 per month and to confirm enrollment on a subset to achieve an enrollment rate of 50% by December 31, 2020.</p><p><strong>Methods: </strong>We used the Institute for Healthcare Improvement's Model for Improvement. Interventions included system changes in partnership with ECE agencies (eg, interactive map of subsidized preschool options, streamlined enrollment forms), case management with families, and population-based approaches to understand families' needs and the program's overall impact. We plotted the number of monthly facilitated referrals and the percentage of referrals enrolled on run and control charts. We used standard probability-based rules to identify special causes.</p><p><strong>Results: </strong>Facilitated referrals increased from 0 to 29 per month and remained above 15. The percentage of enrolled referrals increased from 30% to 74% in 2018, then decreased to 27% in 2020 when childcare availability declined during the pandemic.</p><p><strong>Conclusions: </strong>Our innovative ECE partnership improved access to high-quality ECE. Interventions could be adopted in part or whole by other clinical practices or WIC offices to equitably improve early childhood experiences for low-income families and racial minorities.</p>\",\"PeriodicalId\":74412,\"journal\":{\"name\":\"Pediatric quality & safety\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2023-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/57/c4/pqs-8-e662.PMC10332832.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pediatric quality & safety\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/pq9.0000000000000662\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric quality & safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/pq9.0000000000000662","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
Using Quality Improvement to Design Early Childhood Services Navigation in Primary Care.
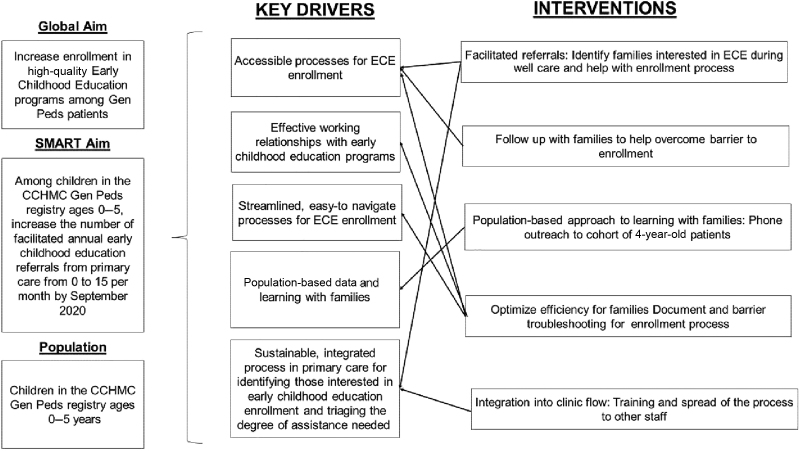
Enrollment in high-quality early childhood education (ECE) improves educational and health outcomes and can mitigate racial and economic disparities. Pediatricians are encouraged to promote ECE yet lack the time and knowledge to assist families effectively. In 2016, our academic primary care center hired an ECE Navigator to promote ECE and help families enroll. Our SMART aims were to increase the number of children with facilitated referrals to high-quality ECE programs from 0 to 15 per month and to confirm enrollment on a subset to achieve an enrollment rate of 50% by December 31, 2020.
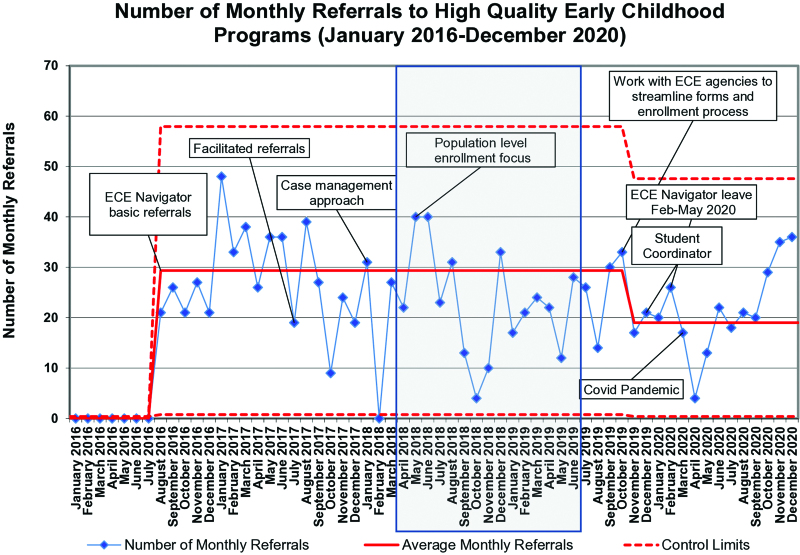
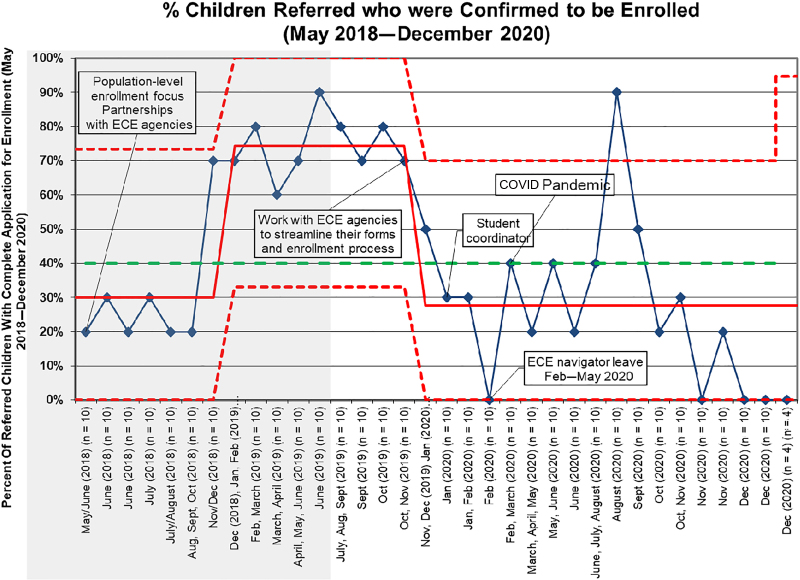
Methods: We used the Institute for Healthcare Improvement's Model for Improvement. Interventions included system changes in partnership with ECE agencies (eg, interactive map of subsidized preschool options, streamlined enrollment forms), case management with families, and population-based approaches to understand families' needs and the program's overall impact. We plotted the number of monthly facilitated referrals and the percentage of referrals enrolled on run and control charts. We used standard probability-based rules to identify special causes.
Results: Facilitated referrals increased from 0 to 29 per month and remained above 15. The percentage of enrolled referrals increased from 30% to 74% in 2018, then decreased to 27% in 2020 when childcare availability declined during the pandemic.
Conclusions: Our innovative ECE partnership improved access to high-quality ECE. Interventions could be adopted in part or whole by other clinical practices or WIC offices to equitably improve early childhood experiences for low-income families and racial minorities.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


