Jun Gyo Gwon, Yong-Pil Cho, Youngjin Han, Jungyo Suh, Seung-Kee Min
{"title":"不经体外循环的肾细胞癌肝上腔静脉肿瘤取栓技术提示。","authors":"Jun Gyo Gwon, Yong-Pil Cho, Youngjin Han, Jungyo Suh, Seung-Kee Min","doi":"10.5758/vsi.230056","DOIUrl":null,"url":null,"abstract":"<p><p>Radical nephrectomy with tumor thrombectomy for advanced renal cell carcinoma is an oncologically relevant approach that can achieve long-term survival even in the presence of distant metastases. However, the surgical techniques pose significant challenges. The objective of this clinical review was to present technical recommendations for tumor thrombectomy in the vena cava to facilitate surgical treatment. Transesophageal echocardiography is required to prepare for this procedure. Cardiopulmonary bypass should be considered when the tumor thrombus has invaded the cardiac chamber and clamping is not feasible because of the inability to milk the intracardiac chamber thrombus in the caudal direction. Prior to performing a cavotomy, it is crucial to clamp the contralateral renal vein and infrarenal and suprahepatic inferior vena cava (IVC). If the suprahepatic IVC is separated from the surrounding tissue, it can be gently pulled down toward the patient's leg until the lower margin of the atrium becomes visible. Subsequently, the tumor thrombus should be carefully pulled downward to a position where it can be clamped. Implementing the Pringle maneuver to reduce blood flow from the hepatic veins to the IVC during IVC cavotomy is simpler than clamping the hepatic veins. Sequential clamping is a two-stage method of dividing thrombectomy by clamping the IVC twice, first suprahepatically and then midretrohepatically. This sequential clamping technique helps minimize hypotension status and the Pringle maneuver time compared to single clamping. Additionally, a spiral cavotomy can decrease the degree of primary closure narrowing. The oncological prognoses of patients can be improved by incorporating these technical recommendations.</p>","PeriodicalId":52311,"journal":{"name":"Vascular Specialist International","volume":"39 ","pages":"23"},"PeriodicalIF":0.8000,"publicationDate":"2023-09-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/32/3e/vsi-39-23.PMC10480049.pdf","citationCount":"0","resultStr":"{\"title\":\"Technical Tips for Performing Suprahepatic Vena Cava Tumor Thrombectomy in Renal Cell Carcinoma without Using Cardiopulmonary Bypass.\",\"authors\":\"Jun Gyo Gwon, Yong-Pil Cho, Youngjin Han, Jungyo Suh, Seung-Kee Min\",\"doi\":\"10.5758/vsi.230056\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Radical nephrectomy with tumor thrombectomy for advanced renal cell carcinoma is an oncologically relevant approach that can achieve long-term survival even in the presence of distant metastases. However, the surgical techniques pose significant challenges. The objective of this clinical review was to present technical recommendations for tumor thrombectomy in the vena cava to facilitate surgical treatment. Transesophageal echocardiography is required to prepare for this procedure. Cardiopulmonary bypass should be considered when the tumor thrombus has invaded the cardiac chamber and clamping is not feasible because of the inability to milk the intracardiac chamber thrombus in the caudal direction. Prior to performing a cavotomy, it is crucial to clamp the contralateral renal vein and infrarenal and suprahepatic inferior vena cava (IVC). If the suprahepatic IVC is separated from the surrounding tissue, it can be gently pulled down toward the patient's leg until the lower margin of the atrium becomes visible. Subsequently, the tumor thrombus should be carefully pulled downward to a position where it can be clamped. Implementing the Pringle maneuver to reduce blood flow from the hepatic veins to the IVC during IVC cavotomy is simpler than clamping the hepatic veins. Sequential clamping is a two-stage method of dividing thrombectomy by clamping the IVC twice, first suprahepatically and then midretrohepatically. This sequential clamping technique helps minimize hypotension status and the Pringle maneuver time compared to single clamping. Additionally, a spiral cavotomy can decrease the degree of primary closure narrowing. The oncological prognoses of patients can be improved by incorporating these technical recommendations.</p>\",\"PeriodicalId\":52311,\"journal\":{\"name\":\"Vascular Specialist International\",\"volume\":\"39 \",\"pages\":\"23\"},\"PeriodicalIF\":0.8000,\"publicationDate\":\"2023-09-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/32/3e/vsi-39-23.PMC10480049.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Vascular Specialist International\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5758/vsi.230056\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"PERIPHERAL VASCULAR DISEASE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Vascular Specialist International","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5758/vsi.230056","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
Technical Tips for Performing Suprahepatic Vena Cava Tumor Thrombectomy in Renal Cell Carcinoma without Using Cardiopulmonary Bypass.
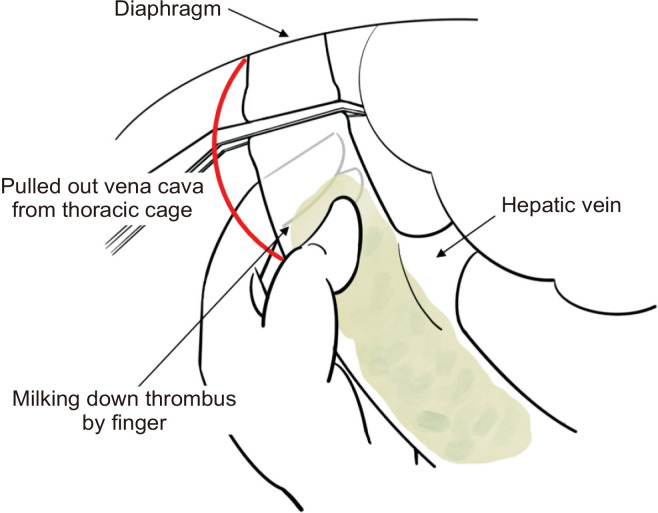
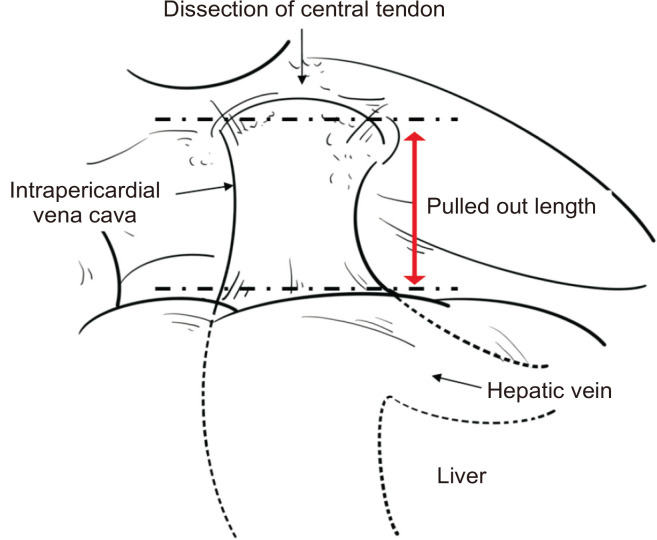
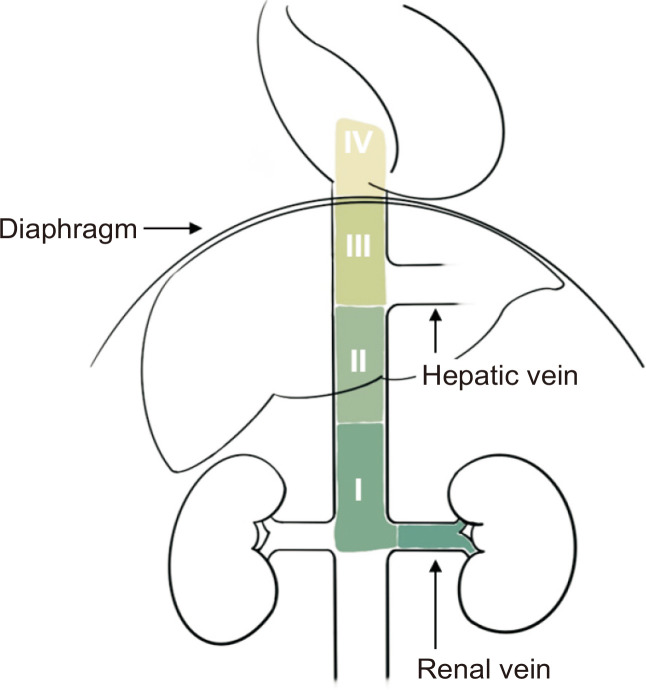
Radical nephrectomy with tumor thrombectomy for advanced renal cell carcinoma is an oncologically relevant approach that can achieve long-term survival even in the presence of distant metastases. However, the surgical techniques pose significant challenges. The objective of this clinical review was to present technical recommendations for tumor thrombectomy in the vena cava to facilitate surgical treatment. Transesophageal echocardiography is required to prepare for this procedure. Cardiopulmonary bypass should be considered when the tumor thrombus has invaded the cardiac chamber and clamping is not feasible because of the inability to milk the intracardiac chamber thrombus in the caudal direction. Prior to performing a cavotomy, it is crucial to clamp the contralateral renal vein and infrarenal and suprahepatic inferior vena cava (IVC). If the suprahepatic IVC is separated from the surrounding tissue, it can be gently pulled down toward the patient's leg until the lower margin of the atrium becomes visible. Subsequently, the tumor thrombus should be carefully pulled downward to a position where it can be clamped. Implementing the Pringle maneuver to reduce blood flow from the hepatic veins to the IVC during IVC cavotomy is simpler than clamping the hepatic veins. Sequential clamping is a two-stage method of dividing thrombectomy by clamping the IVC twice, first suprahepatically and then midretrohepatically. This sequential clamping technique helps minimize hypotension status and the Pringle maneuver time compared to single clamping. Additionally, a spiral cavotomy can decrease the degree of primary closure narrowing. The oncological prognoses of patients can be improved by incorporating these technical recommendations.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


