Ronald A Navarro, Priscilla H Chan, Heather A Prentice, Michael Pearl, Frederick A Matsen Rd, Matthew D McElvany
{"title":"使用术前CT扫描和患者专用仪器可能不能改善肩关节置换术后的短期不良事件:来自大型综合医疗保健系统的结果。","authors":"Ronald A Navarro, Priscilla H Chan, Heather A Prentice, Michael Pearl, Frederick A Matsen Rd, Matthew D McElvany","doi":"10.2106/JBJS.OA.22.00139","DOIUrl":null,"url":null,"abstract":"<p><p>Ongoing innovation leads to a continuous influx of new technologies related to shoulder arthroplasty. These are made available to surgeons and marketed to both health-care providers and patients with the hope of improving outcomes. We sought to evaluate how preoperative planning technologies for shoulder arthroplasty affect outcomes.</p><p><strong>Methods: </strong>This was a retrospective cohort study conducted using data from an integrated health-care system's shoulder arthroplasty registry. Adult patients who underwent primary elective anatomic or reverse total shoulder arthroplasty (2015 to 2020) were identified. Preoperative planning technologies were identified as (1) a computed tomography (CT) scan and (2) patient-specific instrumentation (PSI). Multivariable Cox regression and logistic regression were used to compare the risk of aseptic revision and 90-day adverse events, respectively, between procedures for which technologies were and were not used.</p><p><strong>Results: </strong>The study sample included 8,117 procedures (in 7,372 patients) with an average follow-up of 2.9 years (maximum, 6 years). No reduction in the risk of aseptic revision was observed for patients having either preoperative CT scans (hazard ratio [HR] = 1.22; 95% confidence interval [CI] = 0.87 to 1.72) or PSI (HR = 1.44; 95% CI = 0.71 to 2.92). Patients having CT scans had a lower likelihood of 90-day emergency department visits (odds ratio [OR] = 0.84; 95% CI = 0.73 to 0.97) but a higher likelihood of 90-day venous thromboembolic events (OR = 1.79; 95% CI = 1.18 to 2.74). Patients with PSI use had a higher likelihood of 90-day deep infection (OR = 7.74; 95% CI = 1.11 to 53.94).</p><p><strong>Conclusions: </strong>We found no reduction in the risk of aseptic revision with the use of these technologies. Patients having CT scans and PSI use had a higher likelihood of venous thromboembolism and deep infection, respectively. Ongoing research with extended follow-up is being conducted to further examine the effects of these technologies on patient outcomes.</p><p><strong>Level of evidence: </strong>Diagnostic Level III. See Instructions for Authors for a complete description of levels of evidence.</p>","PeriodicalId":36492,"journal":{"name":"JBJS Open Access","volume":"8 3","pages":""},"PeriodicalIF":2.3000,"publicationDate":"2023-07-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1c/f0/jbjsoa-8-e22.00139.PMC10319369.pdf","citationCount":"0","resultStr":"{\"title\":\"Use of Preoperative CT Scans and Patient-Specific Instrumentation May Not Improve Short-Term Adverse Events After Shoulder Arthroplasty: Results from a Large Integrated Health-Care System.\",\"authors\":\"Ronald A Navarro, Priscilla H Chan, Heather A Prentice, Michael Pearl, Frederick A Matsen Rd, Matthew D McElvany\",\"doi\":\"10.2106/JBJS.OA.22.00139\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Ongoing innovation leads to a continuous influx of new technologies related to shoulder arthroplasty. These are made available to surgeons and marketed to both health-care providers and patients with the hope of improving outcomes. We sought to evaluate how preoperative planning technologies for shoulder arthroplasty affect outcomes.</p><p><strong>Methods: </strong>This was a retrospective cohort study conducted using data from an integrated health-care system's shoulder arthroplasty registry. Adult patients who underwent primary elective anatomic or reverse total shoulder arthroplasty (2015 to 2020) were identified. Preoperative planning technologies were identified as (1) a computed tomography (CT) scan and (2) patient-specific instrumentation (PSI). Multivariable Cox regression and logistic regression were used to compare the risk of aseptic revision and 90-day adverse events, respectively, between procedures for which technologies were and were not used.</p><p><strong>Results: </strong>The study sample included 8,117 procedures (in 7,372 patients) with an average follow-up of 2.9 years (maximum, 6 years). No reduction in the risk of aseptic revision was observed for patients having either preoperative CT scans (hazard ratio [HR] = 1.22; 95% confidence interval [CI] = 0.87 to 1.72) or PSI (HR = 1.44; 95% CI = 0.71 to 2.92). Patients having CT scans had a lower likelihood of 90-day emergency department visits (odds ratio [OR] = 0.84; 95% CI = 0.73 to 0.97) but a higher likelihood of 90-day venous thromboembolic events (OR = 1.79; 95% CI = 1.18 to 2.74). Patients with PSI use had a higher likelihood of 90-day deep infection (OR = 7.74; 95% CI = 1.11 to 53.94).</p><p><strong>Conclusions: </strong>We found no reduction in the risk of aseptic revision with the use of these technologies. Patients having CT scans and PSI use had a higher likelihood of venous thromboembolism and deep infection, respectively. Ongoing research with extended follow-up is being conducted to further examine the effects of these technologies on patient outcomes.</p><p><strong>Level of evidence: </strong>Diagnostic Level III. See Instructions for Authors for a complete description of levels of evidence.</p>\",\"PeriodicalId\":36492,\"journal\":{\"name\":\"JBJS Open Access\",\"volume\":\"8 3\",\"pages\":\"\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2023-07-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1c/f0/jbjsoa-8-e22.00139.PMC10319369.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JBJS Open Access\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2106/JBJS.OA.22.00139\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JBJS Open Access","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2106/JBJS.OA.22.00139","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/7/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
摘要
持续的创新导致与肩关节置换术相关的新技术不断涌入。这些都提供给外科医生,并向保健提供者和患者销售,希望改善结果。我们试图评估肩关节置换术术前计划技术如何影响结果。方法:这是一项回顾性队列研究,使用综合医疗保健系统的肩关节置换术登记处的数据。对2015年至2020年接受初级选择性解剖或反向全肩关节置换术的成年患者进行了研究。术前计划技术确定为(1)计算机断层扫描(CT)和(2)患者特异性仪器(PSI)。多变量Cox回归和logistic回归分别用于比较使用和未使用技术的手术过程中无菌修订和90天不良事件的风险。结果:研究样本包括8,117例手术(7372例患者),平均随访2.9年(最长6年)。术前进行CT扫描的患者未观察到无菌翻修的风险降低(风险比[HR] = 1.22;95%可信区间[CI] = 0.87 ~ 1.72)或PSI (HR = 1.44;95% CI = 0.71 ~ 2.92)。接受CT扫描的患者90天内急诊科就诊的可能性较低(优势比[OR] = 0.84;95% CI = 0.73至0.97),但90天静脉血栓栓塞事件的可能性更高(OR = 1.79;95% CI = 1.18 ~ 2.74)。使用PSI的患者发生90天深部感染的可能性更高(OR = 7.74;95% CI = 1.11 ~ 53.94)。结论:我们发现使用这些技术并没有降低无菌翻修的风险。进行CT扫描和使用PSI的患者分别有更高的可能性发生静脉血栓栓塞和深部感染。目前正在进行长期随访的研究,以进一步检查这些技术对患者预后的影响。证据等级:诊断级III。有关证据水平的完整描述,请参见作者说明。
Use of Preoperative CT Scans and Patient-Specific Instrumentation May Not Improve Short-Term Adverse Events After Shoulder Arthroplasty: Results from a Large Integrated Health-Care System.
Ongoing innovation leads to a continuous influx of new technologies related to shoulder arthroplasty. These are made available to surgeons and marketed to both health-care providers and patients with the hope of improving outcomes. We sought to evaluate how preoperative planning technologies for shoulder arthroplasty affect outcomes.
Methods: This was a retrospective cohort study conducted using data from an integrated health-care system's shoulder arthroplasty registry. Adult patients who underwent primary elective anatomic or reverse total shoulder arthroplasty (2015 to 2020) were identified. Preoperative planning technologies were identified as (1) a computed tomography (CT) scan and (2) patient-specific instrumentation (PSI). Multivariable Cox regression and logistic regression were used to compare the risk of aseptic revision and 90-day adverse events, respectively, between procedures for which technologies were and were not used.
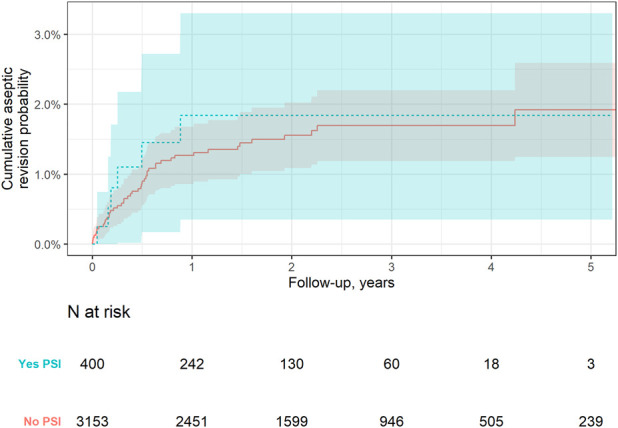
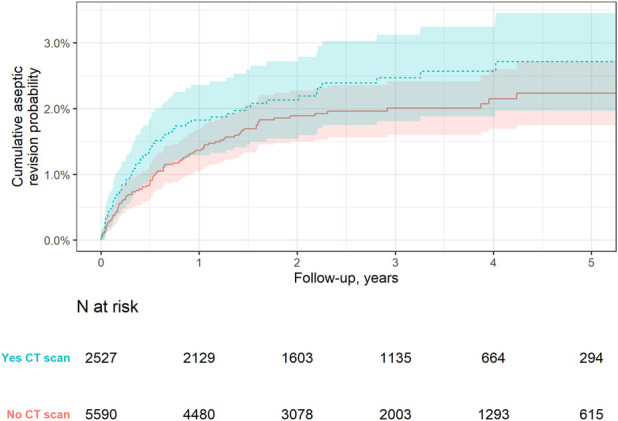
Results: The study sample included 8,117 procedures (in 7,372 patients) with an average follow-up of 2.9 years (maximum, 6 years). No reduction in the risk of aseptic revision was observed for patients having either preoperative CT scans (hazard ratio [HR] = 1.22; 95% confidence interval [CI] = 0.87 to 1.72) or PSI (HR = 1.44; 95% CI = 0.71 to 2.92). Patients having CT scans had a lower likelihood of 90-day emergency department visits (odds ratio [OR] = 0.84; 95% CI = 0.73 to 0.97) but a higher likelihood of 90-day venous thromboembolic events (OR = 1.79; 95% CI = 1.18 to 2.74). Patients with PSI use had a higher likelihood of 90-day deep infection (OR = 7.74; 95% CI = 1.11 to 53.94).
Conclusions: We found no reduction in the risk of aseptic revision with the use of these technologies. Patients having CT scans and PSI use had a higher likelihood of venous thromboembolism and deep infection, respectively. Ongoing research with extended follow-up is being conducted to further examine the effects of these technologies on patient outcomes.
Level of evidence: Diagnostic Level III. See Instructions for Authors for a complete description of levels of evidence.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


