Scott Munro, Debbie Cooke, Mark Joy, Adam Smith, Kurtis Poole, Laurence Perciato, Janet Holah, Ottilia Speirs, Tom Quinn
{"title":"院前12导联心电图与急诊急诊急性卒中患者延迟时间更长和预后更差相关:一项相关队列研究","authors":"Scott Munro, Debbie Cooke, Mark Joy, Adam Smith, Kurtis Poole, Laurence Perciato, Janet Holah, Ottilia Speirs, Tom Quinn","doi":"10.29045/14784726.2022.09.7.2.16","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To investigate the association between pre-hospital 12-lead electrocardiogram (PHECG) use in patients presenting to emergency medical services (EMS) with acute stroke, and clinical outcomes and system delays.</p><p><strong>Methods: </strong>Multi-centre linked cohort study. Patients with verified acute stroke admitted to hospital via EMS were identified through routinely collected hospital data and linked to EMS clinical records via EMS unique identifiers. Ordinal and logistic regression analyses were undertaken to analyse the relationship between having a PHECG and modified Rankin Scale (mRS); hospital mortality; pre-hospital time intervals; door-to-scan and door-to-needle times; and rates of thrombolysis.</p><p><strong>Results: </strong>Of 1161 eligible patients admitted between 29 December 2013 and 30 January 2017, PHECG was performed in 558 (48%). PHECG was associated with an increase in mRS (adjusted odds ratio [aOR] 1.30, 95% confidence interval [CI] 1.01-1.66, p = 0.04) and hospital mortality (aOR 1.83, 95% CI 1.26-2.67, p = 0.002). There was no association between PHECG and administration of thrombolytic treatment (aOR 1.06, 95% CI 0.75-1.52, p = 0.73). Patients who had PHECG recorded spent longer under the care of EMS (median 49 vs 43 minutes, p = 0.006). No difference in times to receiving brain scan (median 28 with PHECG vs 29 minutes no PHECG, p = 0.32) or thrombolysis (median 46 vs 48 minutes, p = 0.37) were observed.</p><p><strong>Conclusion: </strong>The PHECG was associated with worse outcomes and longer delays in patients with acute ischaemic stroke.</p>","PeriodicalId":72470,"journal":{"name":"British paramedic journal","volume":"7 2","pages":"16-23"},"PeriodicalIF":0.0000,"publicationDate":"2022-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9662160/pdf/","citationCount":"3","resultStr":"{\"title\":\"The pre-hospital 12-lead electrocardiogram is associated with longer delay and worse outcomes in patients presenting to emergency medical services with acute stroke: a linked cohort study.\",\"authors\":\"Scott Munro, Debbie Cooke, Mark Joy, Adam Smith, Kurtis Poole, Laurence Perciato, Janet Holah, Ottilia Speirs, Tom Quinn\",\"doi\":\"10.29045/14784726.2022.09.7.2.16\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>To investigate the association between pre-hospital 12-lead electrocardiogram (PHECG) use in patients presenting to emergency medical services (EMS) with acute stroke, and clinical outcomes and system delays.</p><p><strong>Methods: </strong>Multi-centre linked cohort study. Patients with verified acute stroke admitted to hospital via EMS were identified through routinely collected hospital data and linked to EMS clinical records via EMS unique identifiers. Ordinal and logistic regression analyses were undertaken to analyse the relationship between having a PHECG and modified Rankin Scale (mRS); hospital mortality; pre-hospital time intervals; door-to-scan and door-to-needle times; and rates of thrombolysis.</p><p><strong>Results: </strong>Of 1161 eligible patients admitted between 29 December 2013 and 30 January 2017, PHECG was performed in 558 (48%). PHECG was associated with an increase in mRS (adjusted odds ratio [aOR] 1.30, 95% confidence interval [CI] 1.01-1.66, p = 0.04) and hospital mortality (aOR 1.83, 95% CI 1.26-2.67, p = 0.002). There was no association between PHECG and administration of thrombolytic treatment (aOR 1.06, 95% CI 0.75-1.52, p = 0.73). Patients who had PHECG recorded spent longer under the care of EMS (median 49 vs 43 minutes, p = 0.006). No difference in times to receiving brain scan (median 28 with PHECG vs 29 minutes no PHECG, p = 0.32) or thrombolysis (median 46 vs 48 minutes, p = 0.37) were observed.</p><p><strong>Conclusion: </strong>The PHECG was associated with worse outcomes and longer delays in patients with acute ischaemic stroke.</p>\",\"PeriodicalId\":72470,\"journal\":{\"name\":\"British paramedic journal\",\"volume\":\"7 2\",\"pages\":\"16-23\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9662160/pdf/\",\"citationCount\":\"3\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"British paramedic journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.29045/14784726.2022.09.7.2.16\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"British paramedic journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.29045/14784726.2022.09.7.2.16","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 3
摘要
目的:探讨急诊医疗服务(EMS)急性脑卒中患者院前12导联心电图(PHECG)使用与临床结果和系统延迟之间的关系。方法:多中心关联队列研究。通过EMS入院的经证实的急性中风患者通过常规收集的医院数据进行识别,并通过EMS唯一标识符与EMS临床记录相关联。采用序数和逻辑回归分析分析PHECG与改良兰金量表(mRS)之间的关系;医院的死亡率;院前时间间隔;从门到扫描和从门到针的时间;以及溶栓率。结果:在2013年12月29日至2017年1月30日期间入院的1161例符合条件的患者中,558例(48%)进行了PHECG。PHECG与mRS升高(调整比值比[aOR] 1.30, 95%可信区间[CI] 1.01-1.66, p = 0.04)和住院死亡率升高(aOR 1.83, 95% CI 1.26-2.67, p = 0.002)相关。PHECG与溶栓治疗之间无相关性(aOR 1.06, 95% CI 0.75-1.52, p = 0.73)。有PHECG记录的患者接受EMS治疗的时间更长(中位数为49分钟vs 43分钟,p = 0.006)。在接受脑部扫描(有PHECG的中位28分钟vs无PHECG的29分钟,p = 0.32)或溶栓治疗(中位46分钟vs 48分钟,p = 0.37)的时间上没有观察到差异。结论:PHECG与急性缺血性脑卒中患者预后较差、延迟时间较长相关。
The pre-hospital 12-lead electrocardiogram is associated with longer delay and worse outcomes in patients presenting to emergency medical services with acute stroke: a linked cohort study.
Objectives: To investigate the association between pre-hospital 12-lead electrocardiogram (PHECG) use in patients presenting to emergency medical services (EMS) with acute stroke, and clinical outcomes and system delays.
Methods: Multi-centre linked cohort study. Patients with verified acute stroke admitted to hospital via EMS were identified through routinely collected hospital data and linked to EMS clinical records via EMS unique identifiers. Ordinal and logistic regression analyses were undertaken to analyse the relationship between having a PHECG and modified Rankin Scale (mRS); hospital mortality; pre-hospital time intervals; door-to-scan and door-to-needle times; and rates of thrombolysis.
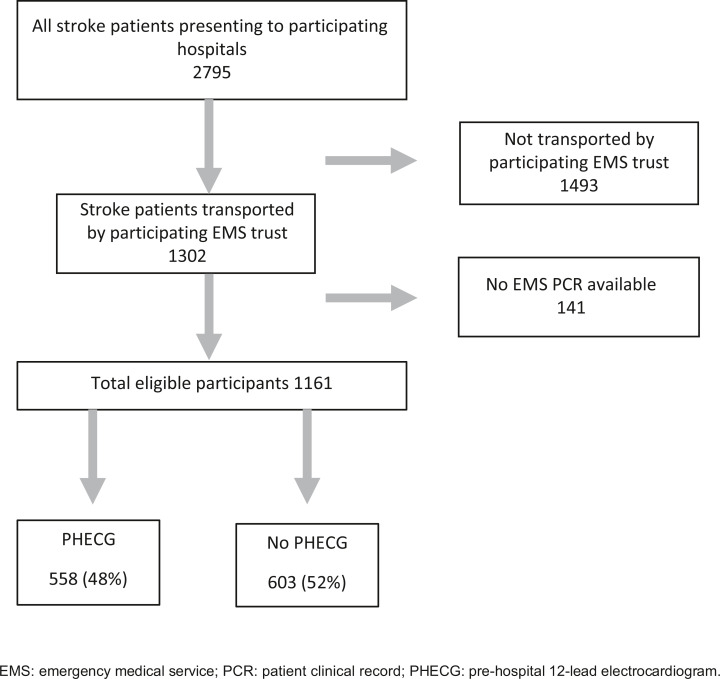
Results: Of 1161 eligible patients admitted between 29 December 2013 and 30 January 2017, PHECG was performed in 558 (48%). PHECG was associated with an increase in mRS (adjusted odds ratio [aOR] 1.30, 95% confidence interval [CI] 1.01-1.66, p = 0.04) and hospital mortality (aOR 1.83, 95% CI 1.26-2.67, p = 0.002). There was no association between PHECG and administration of thrombolytic treatment (aOR 1.06, 95% CI 0.75-1.52, p = 0.73). Patients who had PHECG recorded spent longer under the care of EMS (median 49 vs 43 minutes, p = 0.006). No difference in times to receiving brain scan (median 28 with PHECG vs 29 minutes no PHECG, p = 0.32) or thrombolysis (median 46 vs 48 minutes, p = 0.37) were observed.
Conclusion: The PHECG was associated with worse outcomes and longer delays in patients with acute ischaemic stroke.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


