Emily L Graul, Philip W Stone, Georgie M Massen, Sara Hatam, Alexander Adamson, Spiros Denaxas, Nicholas S Peters, Jennifer K Quint
{"title":"电子医疗记录数据中处方的确定:标准化、可复制药物代码表的开发方法。","authors":"Emily L Graul, Philip W Stone, Georgie M Massen, Sara Hatam, Alexander Adamson, Spiros Denaxas, Nicholas S Peters, Jennifer K Quint","doi":"10.1093/jamiaopen/ooad078","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To develop a standardizable, reproducible method for creating drug codelists that incorporates clinical expertise and is adaptable to other studies and databases.</p><p><strong>Materials and methods: </strong>We developed methods to generate drug codelists and tested this using the Clinical Practice Research Datalink (CPRD) Aurum database, accounting for missing data in the database. We generated codelists for: (1) cardiovascular disease and (2) inhaled Chronic Obstructive Pulmonary Disease (COPD) therapies, applying them to a sample cohort of 335 931 COPD patients. We compared searching all drug dictionary variables (A) against searching only (B) chemical or (C) ontological variables.</p><p><strong>Results: </strong>In Search A, we identified 165 150 patients prescribed cardiovascular drugs (49.2% of cohort), and 317 963 prescribed COPD inhalers (94.7% of cohort). Evaluating output per search strategy, Search C missed numerous prescriptions, including vasodilator anti-hypertensives (A and B:19 696 prescriptions; C:1145) and SAMA inhalers (A and B:35 310; C:564).</p><p><strong>Discussion: </strong>We recommend the full search (A) for comprehensiveness. There are special considerations when generating adaptable and generalizable drug codelists, including fluctuating status, cohort-specific drug indications, underlying hierarchical ontology, and statistical analyses.</p><p><strong>Conclusions: </strong>Methods must have end-to-end clinical input, and be standardizable, reproducible, and understandable to all researchers across data contexts.</p>","PeriodicalId":36278,"journal":{"name":"JAMIA Open","volume":"6 3","pages":"ooad078"},"PeriodicalIF":2.5000,"publicationDate":"2023-08-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d2/17/ooad078.PMC10463548.pdf","citationCount":"0","resultStr":"{\"title\":\"Determining prescriptions in electronic healthcare record data: methods for development of standardized, reproducible drug codelists.\",\"authors\":\"Emily L Graul, Philip W Stone, Georgie M Massen, Sara Hatam, Alexander Adamson, Spiros Denaxas, Nicholas S Peters, Jennifer K Quint\",\"doi\":\"10.1093/jamiaopen/ooad078\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To develop a standardizable, reproducible method for creating drug codelists that incorporates clinical expertise and is adaptable to other studies and databases.</p><p><strong>Materials and methods: </strong>We developed methods to generate drug codelists and tested this using the Clinical Practice Research Datalink (CPRD) Aurum database, accounting for missing data in the database. We generated codelists for: (1) cardiovascular disease and (2) inhaled Chronic Obstructive Pulmonary Disease (COPD) therapies, applying them to a sample cohort of 335 931 COPD patients. We compared searching all drug dictionary variables (A) against searching only (B) chemical or (C) ontological variables.</p><p><strong>Results: </strong>In Search A, we identified 165 150 patients prescribed cardiovascular drugs (49.2% of cohort), and 317 963 prescribed COPD inhalers (94.7% of cohort). Evaluating output per search strategy, Search C missed numerous prescriptions, including vasodilator anti-hypertensives (A and B:19 696 prescriptions; C:1145) and SAMA inhalers (A and B:35 310; C:564).</p><p><strong>Discussion: </strong>We recommend the full search (A) for comprehensiveness. There are special considerations when generating adaptable and generalizable drug codelists, including fluctuating status, cohort-specific drug indications, underlying hierarchical ontology, and statistical analyses.</p><p><strong>Conclusions: </strong>Methods must have end-to-end clinical input, and be standardizable, reproducible, and understandable to all researchers across data contexts.</p>\",\"PeriodicalId\":36278,\"journal\":{\"name\":\"JAMIA Open\",\"volume\":\"6 3\",\"pages\":\"ooad078\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2023-08-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d2/17/ooad078.PMC10463548.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JAMIA Open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/jamiaopen/ooad078\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/10/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAMIA Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jamiaopen/ooad078","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/10/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Determining prescriptions in electronic healthcare record data: methods for development of standardized, reproducible drug codelists.
Objective: To develop a standardizable, reproducible method for creating drug codelists that incorporates clinical expertise and is adaptable to other studies and databases.
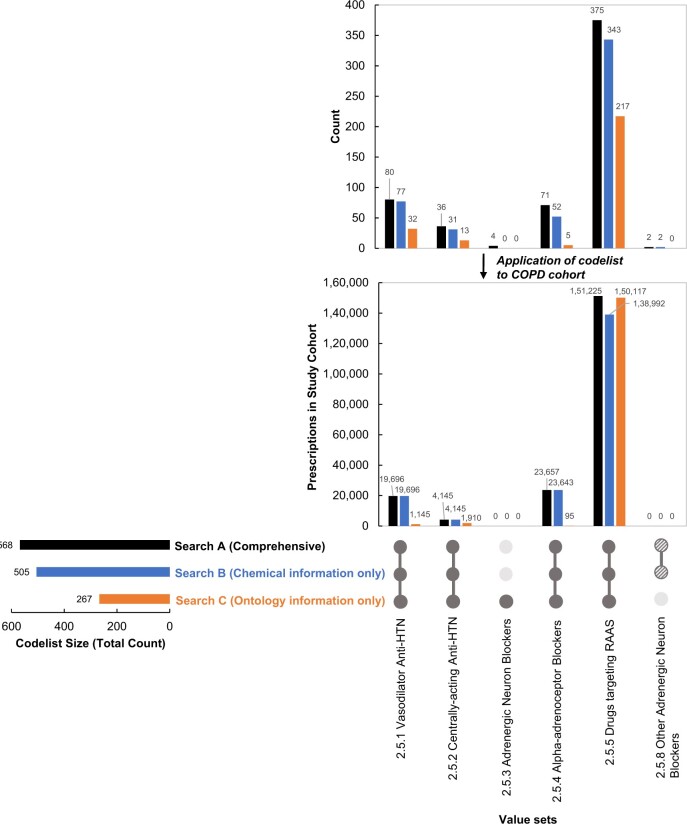
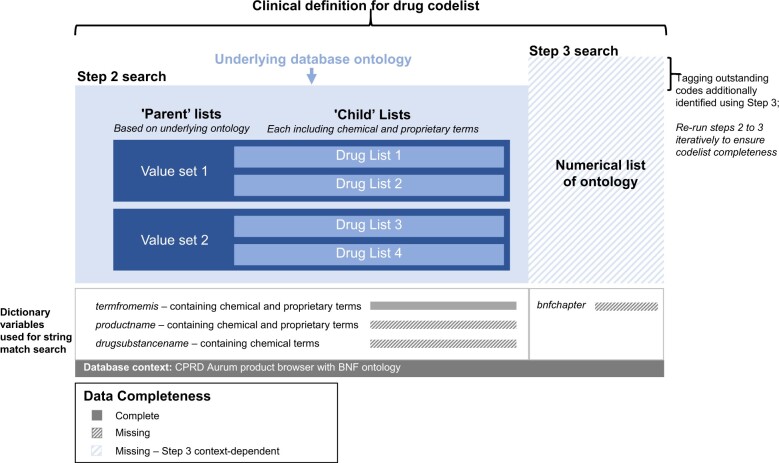
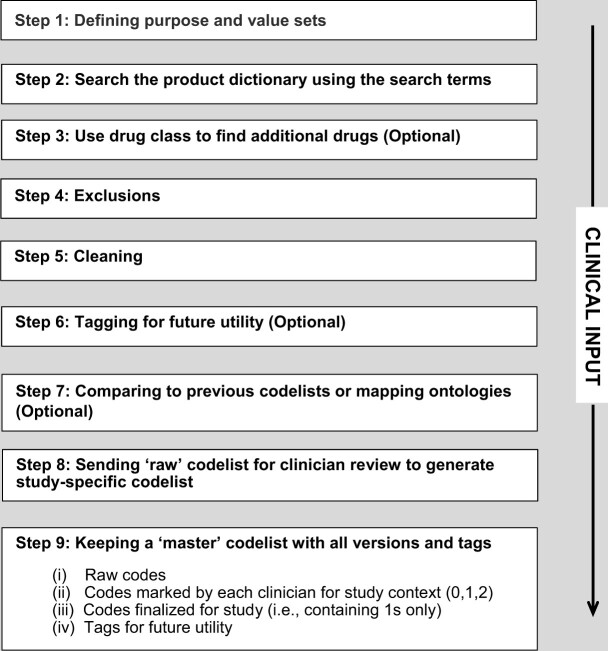
Materials and methods: We developed methods to generate drug codelists and tested this using the Clinical Practice Research Datalink (CPRD) Aurum database, accounting for missing data in the database. We generated codelists for: (1) cardiovascular disease and (2) inhaled Chronic Obstructive Pulmonary Disease (COPD) therapies, applying them to a sample cohort of 335 931 COPD patients. We compared searching all drug dictionary variables (A) against searching only (B) chemical or (C) ontological variables.
Results: In Search A, we identified 165 150 patients prescribed cardiovascular drugs (49.2% of cohort), and 317 963 prescribed COPD inhalers (94.7% of cohort). Evaluating output per search strategy, Search C missed numerous prescriptions, including vasodilator anti-hypertensives (A and B:19 696 prescriptions; C:1145) and SAMA inhalers (A and B:35 310; C:564).
Discussion: We recommend the full search (A) for comprehensiveness. There are special considerations when generating adaptable and generalizable drug codelists, including fluctuating status, cohort-specific drug indications, underlying hierarchical ontology, and statistical analyses.
Conclusions: Methods must have end-to-end clinical input, and be standardizable, reproducible, and understandable to all researchers across data contexts.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


