{"title":"巨大窦房结动脉瘤伴右心房瘘管部分切除及切除1例。","authors":"Usha Kumari, Mansoor Rahman, Muneeb Ullah Jan, Salecah Rahmat Ullah, Fakhar Abbas, Zara Shirazi, Salim Surani","doi":"10.18502/jthc.v18i2.13325","DOIUrl":null,"url":null,"abstract":"<p><p>Coronary artery aneurysms (CAAs) occur when an artery dilates 1.5 times the reference vessel. They occur most commonly because of atherosclerosis. CAAs are a rare phenomenon, and it is even rarer to find a giant CAA, which is roughly defined as a size 400% above the reference vessel. Giant CAAs are commonly found in the right coronary artery. The sinoatrial nodal artery (SNA) is among the least common sites for CAA involvement. Sometimes, communication exists between the aneurysm and a chamber of the heart or a great vessel. The consequences of the fistula depend on its size. Because of the rarity of the condition, guidelines are not well developed. However, small CAAs can be managed conservatively, whereas giant CAAs require resection, ligation, and bypass grafting. CAAs have a predilection for males and the elderly. We describe a 40-year-old South Asian woman presenting with mild dyspnea on exertion of 1 year's duration. Echocardiography showed a 60×60 mm cystic sac, subsequently confirmed by computerized tomography, which showed 3 large aneurysms (70×61 mm) and 3 small aneurysms in the SNA. Coronary angiography illustrated that the SNA branched off the left main coronary artery, and the aneurysm communicated with the right coronary artery. The aneurysm was partially resected and plicated.</p>","PeriodicalId":39149,"journal":{"name":"Journal of Tehran University Heart Center","volume":"18 2","pages":"142-145"},"PeriodicalIF":0.0000,"publicationDate":"2023-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ed/81/JTHC-18-142.PMC10459341.pdf","citationCount":"0","resultStr":"{\"title\":\"Giant Sinoatrial Nodal Artery Aneurysm with Fistula into the Right Atrium Treated by Partial Resection and Plication: A Case Report.\",\"authors\":\"Usha Kumari, Mansoor Rahman, Muneeb Ullah Jan, Salecah Rahmat Ullah, Fakhar Abbas, Zara Shirazi, Salim Surani\",\"doi\":\"10.18502/jthc.v18i2.13325\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Coronary artery aneurysms (CAAs) occur when an artery dilates 1.5 times the reference vessel. They occur most commonly because of atherosclerosis. CAAs are a rare phenomenon, and it is even rarer to find a giant CAA, which is roughly defined as a size 400% above the reference vessel. Giant CAAs are commonly found in the right coronary artery. The sinoatrial nodal artery (SNA) is among the least common sites for CAA involvement. Sometimes, communication exists between the aneurysm and a chamber of the heart or a great vessel. The consequences of the fistula depend on its size. Because of the rarity of the condition, guidelines are not well developed. However, small CAAs can be managed conservatively, whereas giant CAAs require resection, ligation, and bypass grafting. CAAs have a predilection for males and the elderly. We describe a 40-year-old South Asian woman presenting with mild dyspnea on exertion of 1 year's duration. Echocardiography showed a 60×60 mm cystic sac, subsequently confirmed by computerized tomography, which showed 3 large aneurysms (70×61 mm) and 3 small aneurysms in the SNA. Coronary angiography illustrated that the SNA branched off the left main coronary artery, and the aneurysm communicated with the right coronary artery. The aneurysm was partially resected and plicated.</p>\",\"PeriodicalId\":39149,\"journal\":{\"name\":\"Journal of Tehran University Heart Center\",\"volume\":\"18 2\",\"pages\":\"142-145\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ed/81/JTHC-18-142.PMC10459341.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Tehran University Heart Center\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.18502/jthc.v18i2.13325\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Tehran University Heart Center","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.18502/jthc.v18i2.13325","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
Giant Sinoatrial Nodal Artery Aneurysm with Fistula into the Right Atrium Treated by Partial Resection and Plication: A Case Report.
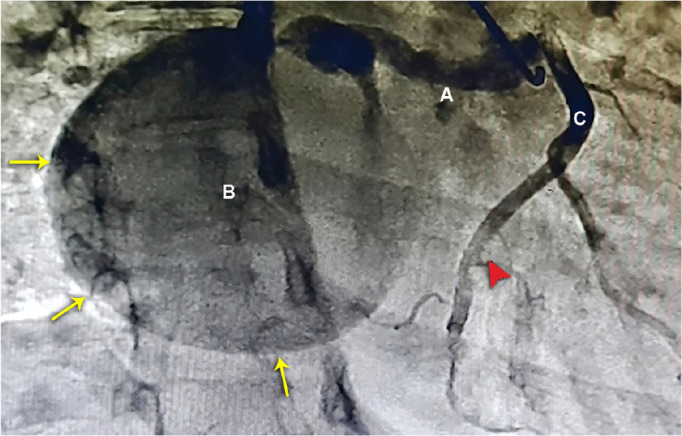
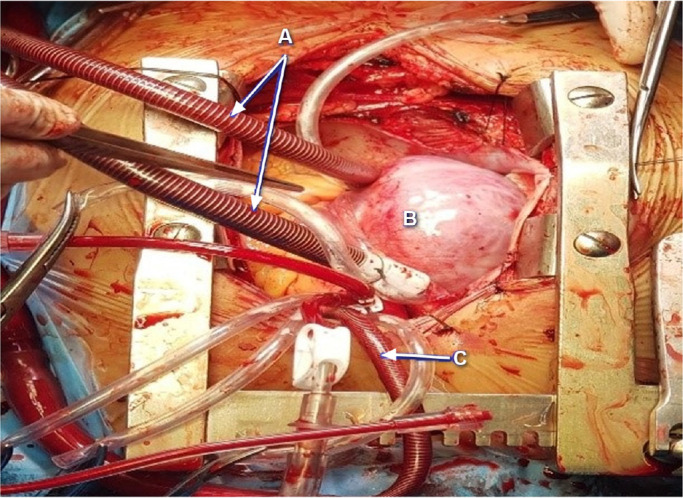
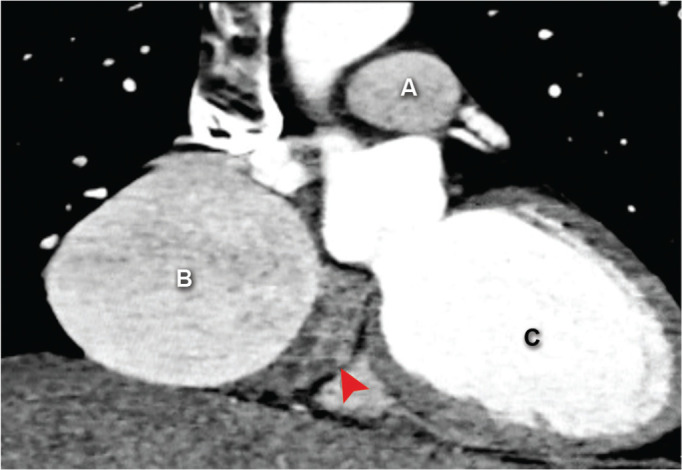
Coronary artery aneurysms (CAAs) occur when an artery dilates 1.5 times the reference vessel. They occur most commonly because of atherosclerosis. CAAs are a rare phenomenon, and it is even rarer to find a giant CAA, which is roughly defined as a size 400% above the reference vessel. Giant CAAs are commonly found in the right coronary artery. The sinoatrial nodal artery (SNA) is among the least common sites for CAA involvement. Sometimes, communication exists between the aneurysm and a chamber of the heart or a great vessel. The consequences of the fistula depend on its size. Because of the rarity of the condition, guidelines are not well developed. However, small CAAs can be managed conservatively, whereas giant CAAs require resection, ligation, and bypass grafting. CAAs have a predilection for males and the elderly. We describe a 40-year-old South Asian woman presenting with mild dyspnea on exertion of 1 year's duration. Echocardiography showed a 60×60 mm cystic sac, subsequently confirmed by computerized tomography, which showed 3 large aneurysms (70×61 mm) and 3 small aneurysms in the SNA. Coronary angiography illustrated that the SNA branched off the left main coronary artery, and the aneurysm communicated with the right coronary artery. The aneurysm was partially resected and plicated.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


