Joaquin Pérez, Matías Accoce, Javier H Dorado, Daniela I Gilgado, Emiliano Navarro, Gimena P Cardoso, Irene Telias, Pablo O Rodriguez, Laurent Brochard
{"title":"低氧性呼吸衰竭患者自发觉醒后首次过渡到压力支持通气失败:COVID-19的影响","authors":"Joaquin Pérez, Matías Accoce, Javier H Dorado, Daniela I Gilgado, Emiliano Navarro, Gimena P Cardoso, Irene Telias, Pablo O Rodriguez, Laurent Brochard","doi":"10.1097/CCE.0000000000000968","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To describe the rate of failure of the first transition to pressure support ventilation (PSV) after systematic spontaneous awakening trials (SATs) in patients with acute hypoxemic respiratory failure (AHRF) and to assess whether the failure is higher in COVID-19 compared with AHRF of other etiologies. To determine predictors and potential association of failure with outcomes.</p><p><strong>Design: </strong>Retrospective cohort study.</p><p><strong>Setting: </strong>Twenty-eight-bedded medical-surgical ICU in a private hospital (Argentina).</p><p><strong>Patients: </strong>Subjects with arterial pressure of oxygen (AHRF to Fio<sub>2</sub> [Pao<sub>2</sub>/Fio<sub>2</sub>] < 300 mm Hg) of different etiologies under controlled mechanical ventilation (MV).</p><p><strong>Interventions: </strong>None.</p><p><strong>Measurements and main results: </strong>We collected data during controlled ventilation within 24 hours before SAT followed by the first PSV transition. Failure was defined as the need to return to fully controlled MV within 3 calendar days of PSV start. A total of 274 patients with AHRF (189 COVID-19 and 85 non-COVID-19) were included. The failure occurred in 120 of 274 subjects (43.7%) and was higher in COVID-19 versus non-COVID-19 (49.7% and 30.5%; <i>p</i> = 0.003). COVID-19 diagnosis (odds ratio [OR]: 2.22; 95% CI [1.15-4.43]; <i>p</i> = 0.020), previous neuromuscular blockers (OR: 2.16; 95% CI [1.15-4.11]; <i>p</i> = 0.017) and higher fentanyl dose (OR: 1.29; 95% CI [1.05-1.60]; <i>p</i> = 0.018) increased the failure chances. Higher BMI (OR: 0.95; 95% CI [0.91-0.99]; <i>p</i> = 0.029), Pao<sub>2</sub>/Fio<sub>2</sub> (OR: 0.87; 95% CI [0.78-0.97]; <i>p</i> = 0.017), and pH (OR: 0.61; 95% CI [0.38-0.96]; <i>p</i> = 0.035) were protective. Failure groups had higher 60-day ventilator dependence (<i>p</i> < 0.001), MV duration (<i>p</i> < 0.0001), and ICU stay (<i>p</i> = 0.001). Patients who failed had higher mortality in COVID-19 group (<i>p</i> < 0.001) but not in the non-COVID-19 (<i>p</i> = 0.083).</p><p><strong>Conclusions: </strong>In patients with AHRF of different etiologies, the failure of the first PSV attempt was 43.7%, and at a higher rate in COVID-19. Independent risk factors included COVID-19 diagnosis, fentanyl dose, previous neuromuscular blockers, acidosis and hypoxemia preceding SAT, whereas higher BMI was protective. Failure was associated with worse outcomes.</p>","PeriodicalId":10759,"journal":{"name":"Critical Care Explorations","volume":"5 9","pages":"e0968"},"PeriodicalIF":0.0000,"publicationDate":"2023-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d9/d6/cc9-5-e0968.PMC10461949.pdf","citationCount":"0","resultStr":"{\"title\":\"Failure of First Transition to Pressure Support Ventilation After Spontaneous Awakening Trials in Hypoxemic Respiratory Failure: Influence of COVID-19.\",\"authors\":\"Joaquin Pérez, Matías Accoce, Javier H Dorado, Daniela I Gilgado, Emiliano Navarro, Gimena P Cardoso, Irene Telias, Pablo O Rodriguez, Laurent Brochard\",\"doi\":\"10.1097/CCE.0000000000000968\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>To describe the rate of failure of the first transition to pressure support ventilation (PSV) after systematic spontaneous awakening trials (SATs) in patients with acute hypoxemic respiratory failure (AHRF) and to assess whether the failure is higher in COVID-19 compared with AHRF of other etiologies. To determine predictors and potential association of failure with outcomes.</p><p><strong>Design: </strong>Retrospective cohort study.</p><p><strong>Setting: </strong>Twenty-eight-bedded medical-surgical ICU in a private hospital (Argentina).</p><p><strong>Patients: </strong>Subjects with arterial pressure of oxygen (AHRF to Fio<sub>2</sub> [Pao<sub>2</sub>/Fio<sub>2</sub>] < 300 mm Hg) of different etiologies under controlled mechanical ventilation (MV).</p><p><strong>Interventions: </strong>None.</p><p><strong>Measurements and main results: </strong>We collected data during controlled ventilation within 24 hours before SAT followed by the first PSV transition. Failure was defined as the need to return to fully controlled MV within 3 calendar days of PSV start. A total of 274 patients with AHRF (189 COVID-19 and 85 non-COVID-19) were included. The failure occurred in 120 of 274 subjects (43.7%) and was higher in COVID-19 versus non-COVID-19 (49.7% and 30.5%; <i>p</i> = 0.003). COVID-19 diagnosis (odds ratio [OR]: 2.22; 95% CI [1.15-4.43]; <i>p</i> = 0.020), previous neuromuscular blockers (OR: 2.16; 95% CI [1.15-4.11]; <i>p</i> = 0.017) and higher fentanyl dose (OR: 1.29; 95% CI [1.05-1.60]; <i>p</i> = 0.018) increased the failure chances. Higher BMI (OR: 0.95; 95% CI [0.91-0.99]; <i>p</i> = 0.029), Pao<sub>2</sub>/Fio<sub>2</sub> (OR: 0.87; 95% CI [0.78-0.97]; <i>p</i> = 0.017), and pH (OR: 0.61; 95% CI [0.38-0.96]; <i>p</i> = 0.035) were protective. Failure groups had higher 60-day ventilator dependence (<i>p</i> < 0.001), MV duration (<i>p</i> < 0.0001), and ICU stay (<i>p</i> = 0.001). Patients who failed had higher mortality in COVID-19 group (<i>p</i> < 0.001) but not in the non-COVID-19 (<i>p</i> = 0.083).</p><p><strong>Conclusions: </strong>In patients with AHRF of different etiologies, the failure of the first PSV attempt was 43.7%, and at a higher rate in COVID-19. Independent risk factors included COVID-19 diagnosis, fentanyl dose, previous neuromuscular blockers, acidosis and hypoxemia preceding SAT, whereas higher BMI was protective. Failure was associated with worse outcomes.</p>\",\"PeriodicalId\":10759,\"journal\":{\"name\":\"Critical Care Explorations\",\"volume\":\"5 9\",\"pages\":\"e0968\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d9/d6/cc9-5-e0968.PMC10461949.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical Care Explorations\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/CCE.0000000000000968\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Care Explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000000968","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
目的:描述急性低氧性呼吸衰竭(AHRF)患者在系统自发觉醒试验(SATs)后首次过渡到压力支持通气(PSV)的失败率,并评估COVID-19患者的失败率是否高于其他病因的AHRF患者。确定失败与结果的预测因素和潜在关联。设计:回顾性队列研究。环境:一家私人医院(阿根廷)设有28张床位的内科-外科ICU。患者:受控机械通气(MV)下不同病因的动脉氧压(AHRF to Fio2 [Pao2/Fio2] < 300 mm Hg)受试者。干预措施:没有。测量和主要结果:我们收集了在SAT前24小时内控制通气期间的数据,随后是第一次PSV过渡。失败被定义为需要在PSV开始后的3个日历天内返回到完全控制的MV。共纳入274例AHRF患者(189例COVID-19, 85例非COVID-19)。274名受试者中有120人(43.7%)失败,COVID-19患者的失败率高于非COVID-19患者(49.7%和30.5%);P = 0.003)。COVID-19诊断(优势比[OR]: 2.22;95% ci [1.15-4.43];p = 0.020),既往神经肌肉阻滞剂(OR: 2.16;95% ci [1.15-4.11];p = 0.017)和较高芬太尼剂量(OR: 1.29;95% ci [1.05-1.60];P = 0.018)增加了失败的机会。较高的BMI (OR: 0.95;95% ci [0.91-0.99];p = 0.029), Pao2/Fio2 (OR: 0.87;95% ci [0.78-0.97];p = 0.017), pH值(OR: 0.61;95% ci [0.38-0.96];P = 0.035)具有保护作用。失败组60天呼吸机依赖性(p < 0.001)、MV持续时间(p < 0.0001)和ICU住院时间(p = 0.001)较高。失败患者的死亡率在COVID-19组较高(p < 0.001),而在非COVID-19组无此差异(p = 0.083)。结论:在不同病因的AHRF患者中,首次PSV尝试的失败率为43.7%,COVID-19患者的失败率更高。独立危险因素包括COVID-19诊断、芬太尼剂量、既往神经肌肉阻滞剂、酸中毒和SAT前低氧血症,而较高的BMI具有保护作用。失败与更糟糕的结果相关。
Failure of First Transition to Pressure Support Ventilation After Spontaneous Awakening Trials in Hypoxemic Respiratory Failure: Influence of COVID-19.
Objectives: To describe the rate of failure of the first transition to pressure support ventilation (PSV) after systematic spontaneous awakening trials (SATs) in patients with acute hypoxemic respiratory failure (AHRF) and to assess whether the failure is higher in COVID-19 compared with AHRF of other etiologies. To determine predictors and potential association of failure with outcomes.
Design: Retrospective cohort study.
Setting: Twenty-eight-bedded medical-surgical ICU in a private hospital (Argentina).
Patients: Subjects with arterial pressure of oxygen (AHRF to Fio2 [Pao2/Fio2] < 300 mm Hg) of different etiologies under controlled mechanical ventilation (MV).
Interventions: None.
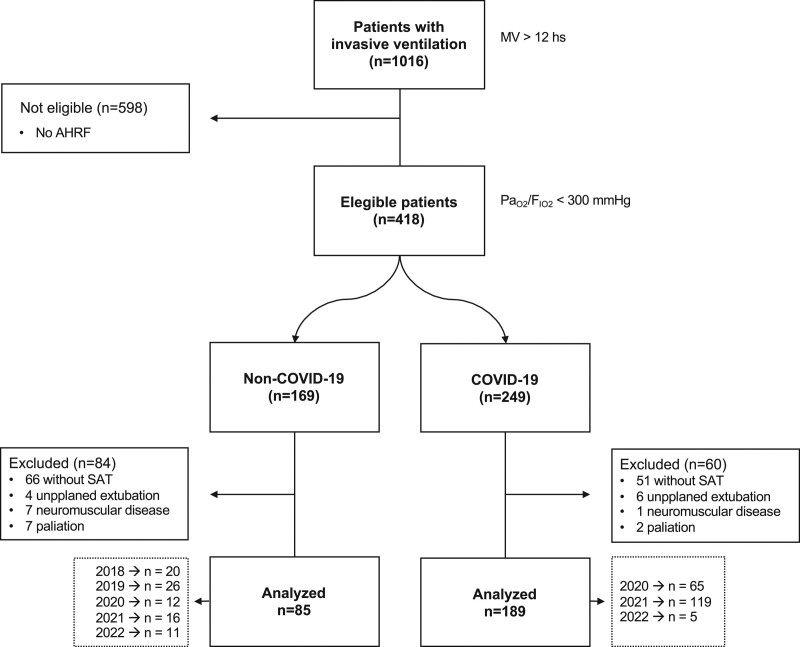
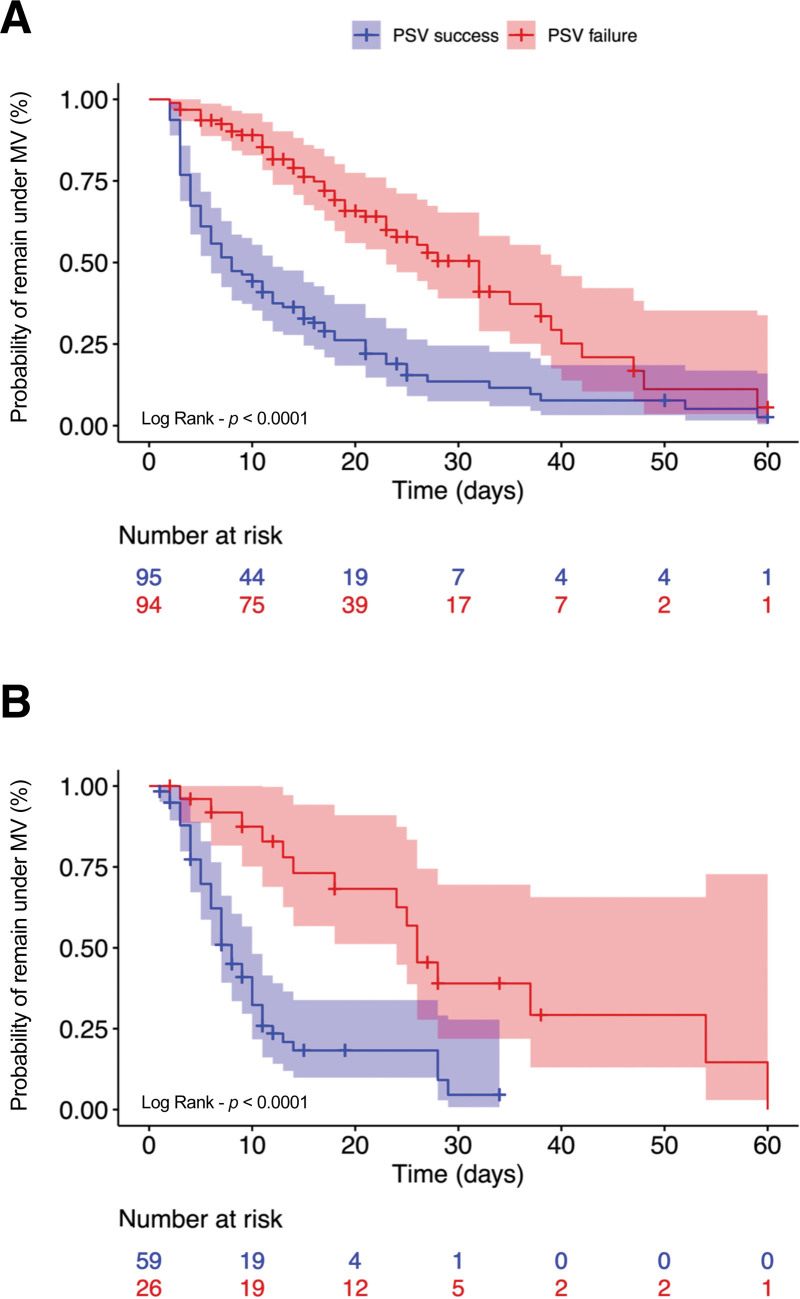
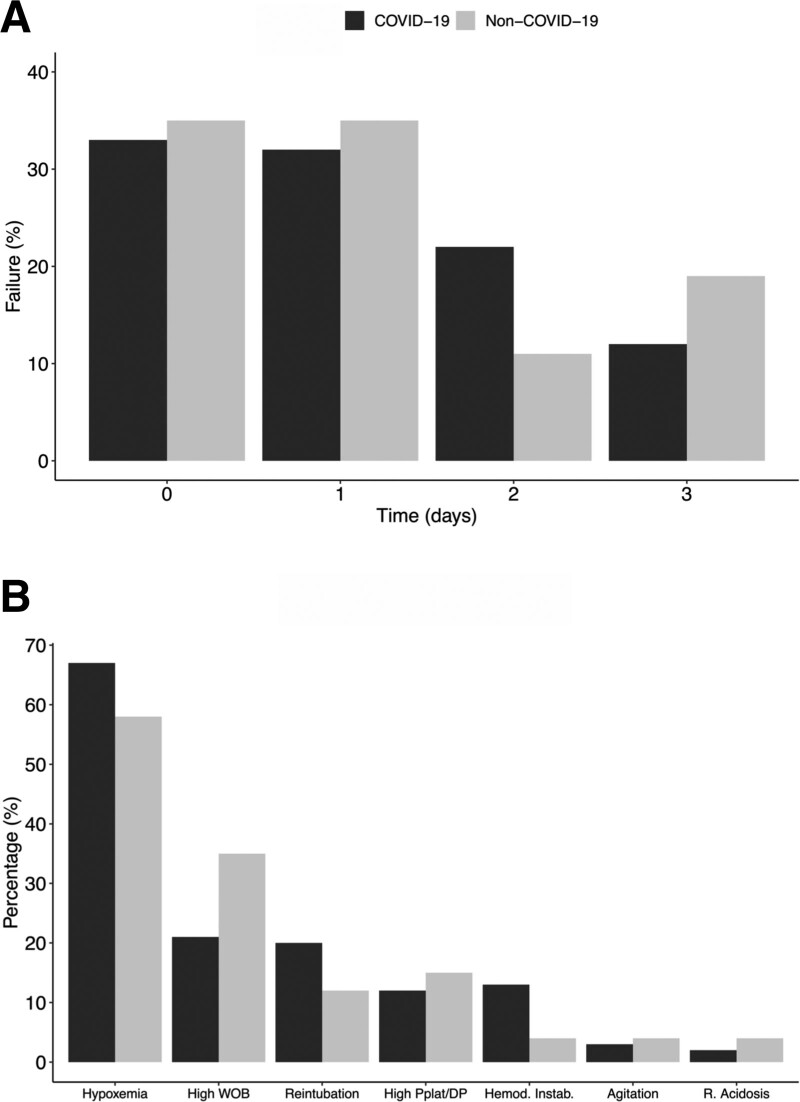
Measurements and main results: We collected data during controlled ventilation within 24 hours before SAT followed by the first PSV transition. Failure was defined as the need to return to fully controlled MV within 3 calendar days of PSV start. A total of 274 patients with AHRF (189 COVID-19 and 85 non-COVID-19) were included. The failure occurred in 120 of 274 subjects (43.7%) and was higher in COVID-19 versus non-COVID-19 (49.7% and 30.5%; p = 0.003). COVID-19 diagnosis (odds ratio [OR]: 2.22; 95% CI [1.15-4.43]; p = 0.020), previous neuromuscular blockers (OR: 2.16; 95% CI [1.15-4.11]; p = 0.017) and higher fentanyl dose (OR: 1.29; 95% CI [1.05-1.60]; p = 0.018) increased the failure chances. Higher BMI (OR: 0.95; 95% CI [0.91-0.99]; p = 0.029), Pao2/Fio2 (OR: 0.87; 95% CI [0.78-0.97]; p = 0.017), and pH (OR: 0.61; 95% CI [0.38-0.96]; p = 0.035) were protective. Failure groups had higher 60-day ventilator dependence (p < 0.001), MV duration (p < 0.0001), and ICU stay (p = 0.001). Patients who failed had higher mortality in COVID-19 group (p < 0.001) but not in the non-COVID-19 (p = 0.083).
Conclusions: In patients with AHRF of different etiologies, the failure of the first PSV attempt was 43.7%, and at a higher rate in COVID-19. Independent risk factors included COVID-19 diagnosis, fentanyl dose, previous neuromuscular blockers, acidosis and hypoxemia preceding SAT, whereas higher BMI was protective. Failure was associated with worse outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


