Ben Gelbart, Sudeep Kumar Kapalavai, Vanessa Marchesini, Jeffrey Presneill, Andrea Veysey, Alyssa Serratore, Jessica Appleyard, Rinaldo Bellomo, Warwick Butt, Trevor Duke
{"title":"用于量化重症监护中机械通气先天性心脏病患儿水肿的临床评分。","authors":"Ben Gelbart, Sudeep Kumar Kapalavai, Vanessa Marchesini, Jeffrey Presneill, Andrea Veysey, Alyssa Serratore, Jessica Appleyard, Rinaldo Bellomo, Warwick Butt, Trevor Duke","doi":"10.1097/CCE.0000000000000924","DOIUrl":null,"url":null,"abstract":"<p><p>Standardized clinical measurements of edema do not exist.</p><p><strong>Objectives: </strong>To describe a 19-point clinical edema score (CES), investigate its interobserver agreement, and compare changes between such CES and body weight.</p><p><strong>Design setting and participants: </strong>Prospective observational study in a tertiary PICU of mechanically ventilated children with congenital heart disease.</p><p><strong>Main outcomes and measures: </strong>Differences in the median CES between observer groups.</p><p><strong>Results: </strong>We studied 61 children, with a median age of 8.0 days (interquartile range, 1.0-14.0 d). A total of 539 CES were performed by three observer groups (medical 1 [reference], medical 2, and bedside nurse) at 0, 24, and 48 hours from enrollment. Overall, there was close agreement between observer groups in mean, median, and upper quartile of CES scores, with least agreement observed in the lower quartile of scores. Across all quartiles of CES, after adjusting for baseline weight, cardiac surgical risk, duration of cardiopulmonary bypass, or peritoneal dialysis during the study, observer groups returned similar mean scores (medical 2: 25th centile +0.1 [95% CI, -0.2 to 0.5], median +0.6 [95% CI, -0.4 to 1.5], 75th centile +0.1 [95% CI, -1.1 to 1.4] and nurse: 25th centile +0.5 [95% CI, 0.0-0.9], median +0.7 [95% CI, 0.0-1.5], 75th centile -0.2 [95% CI, -1.3 to 1.0]) Within a multivariable mixed-effects linear regression model, including adjustment for baseline CES, each 1 point increase in CES was associated with a 12.1 grams (95% CI, 3.2-21 grams) increase in body weight.</p><p><strong>Conclusions and relevance: </strong>In mechanically ventilated children with congenital heart disease, three groups of observers tended to agree when assessing overall edema using an ordinal clinical score assessed in six body regions, with agreement least at low edema scores. An increase in CES was associated with an increase in body weight, suggesting some validity for quantifying edema. Further exploration of the CES as a rapid clinical tool is indicated.</p>","PeriodicalId":10759,"journal":{"name":"Critical Care Explorations","volume":"5 6","pages":"e0924"},"PeriodicalIF":0.0000,"publicationDate":"2023-06-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/2f/da/cc9-5-e0924.PMC10456982.pdf","citationCount":"0","resultStr":"{\"title\":\"A Clinical Score for Quantifying Edema in Mechanically Ventilated Children With Congenital Heart Disease in Intensive Care.\",\"authors\":\"Ben Gelbart, Sudeep Kumar Kapalavai, Vanessa Marchesini, Jeffrey Presneill, Andrea Veysey, Alyssa Serratore, Jessica Appleyard, Rinaldo Bellomo, Warwick Butt, Trevor Duke\",\"doi\":\"10.1097/CCE.0000000000000924\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Standardized clinical measurements of edema do not exist.</p><p><strong>Objectives: </strong>To describe a 19-point clinical edema score (CES), investigate its interobserver agreement, and compare changes between such CES and body weight.</p><p><strong>Design setting and participants: </strong>Prospective observational study in a tertiary PICU of mechanically ventilated children with congenital heart disease.</p><p><strong>Main outcomes and measures: </strong>Differences in the median CES between observer groups.</p><p><strong>Results: </strong>We studied 61 children, with a median age of 8.0 days (interquartile range, 1.0-14.0 d). A total of 539 CES were performed by three observer groups (medical 1 [reference], medical 2, and bedside nurse) at 0, 24, and 48 hours from enrollment. Overall, there was close agreement between observer groups in mean, median, and upper quartile of CES scores, with least agreement observed in the lower quartile of scores. Across all quartiles of CES, after adjusting for baseline weight, cardiac surgical risk, duration of cardiopulmonary bypass, or peritoneal dialysis during the study, observer groups returned similar mean scores (medical 2: 25th centile +0.1 [95% CI, -0.2 to 0.5], median +0.6 [95% CI, -0.4 to 1.5], 75th centile +0.1 [95% CI, -1.1 to 1.4] and nurse: 25th centile +0.5 [95% CI, 0.0-0.9], median +0.7 [95% CI, 0.0-1.5], 75th centile -0.2 [95% CI, -1.3 to 1.0]) Within a multivariable mixed-effects linear regression model, including adjustment for baseline CES, each 1 point increase in CES was associated with a 12.1 grams (95% CI, 3.2-21 grams) increase in body weight.</p><p><strong>Conclusions and relevance: </strong>In mechanically ventilated children with congenital heart disease, three groups of observers tended to agree when assessing overall edema using an ordinal clinical score assessed in six body regions, with agreement least at low edema scores. An increase in CES was associated with an increase in body weight, suggesting some validity for quantifying edema. Further exploration of the CES as a rapid clinical tool is indicated.</p>\",\"PeriodicalId\":10759,\"journal\":{\"name\":\"Critical Care Explorations\",\"volume\":\"5 6\",\"pages\":\"e0924\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-06-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/2f/da/cc9-5-e0924.PMC10456982.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical Care Explorations\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/CCE.0000000000000924\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/6/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Care Explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000000924","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/6/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
目前还没有标准化的临床水肿测量方法:描述19点临床水肿评分(CES),研究其观察者间的一致性,并比较CES与体重之间的变化:主要结果和测量指标:主要结果和测量指标:观察组之间 CES 中位数的差异:我们对61名儿童进行了研究,他们的中位年龄为8.0天(四分位间范围为1.0-14.0天)。三个观察组(医护 1 [参考]、医护 2 和床旁护士)在入院后 0、24 和 48 小时内共进行了 539 次 CES。总体而言,各观察组之间在 CES 评分的平均值、中位数和上四分位数上的一致性非常接近,而在下四分位数上的一致性最低。在对基线体重、心脏手术风险、心肺旁路持续时间或研究期间腹膜透析进行调整后,CES 的所有四分位数中,观察者组的平均得分相似(医护 2:第 25 百分位数 +0.1 [95% CI, -0.2 to 0.5],中位数 +0.6 [95% CI, -0.4 to 1.5],第 75 百分位数 +0.1 [95% CI, -1.1 to 1.4];护士:第 25 百分位数 +0.1 [95% CI, -0.2 to 0.5],中位数 +0.6 [95% CI, -0.4 to 1.5]。在多变量混合效应线性回归模型中,包括对基线 CES 的调整,CES 每增加 1 个点,体重就会增加 12.1 克(95% CI,3.2-21 克):在患有先天性心脏病的机械通气患儿中,三组观察者在使用对身体六个区域进行评估的序数临床评分来评估总体水肿时往往意见一致,在低水肿评分时意见最不一致。CES的增加与体重的增加有关,这表明量化水肿具有一定的有效性。将 CES 作为一种快速临床工具进行进一步探索是有必要的。
A Clinical Score for Quantifying Edema in Mechanically Ventilated Children With Congenital Heart Disease in Intensive Care.
Standardized clinical measurements of edema do not exist.
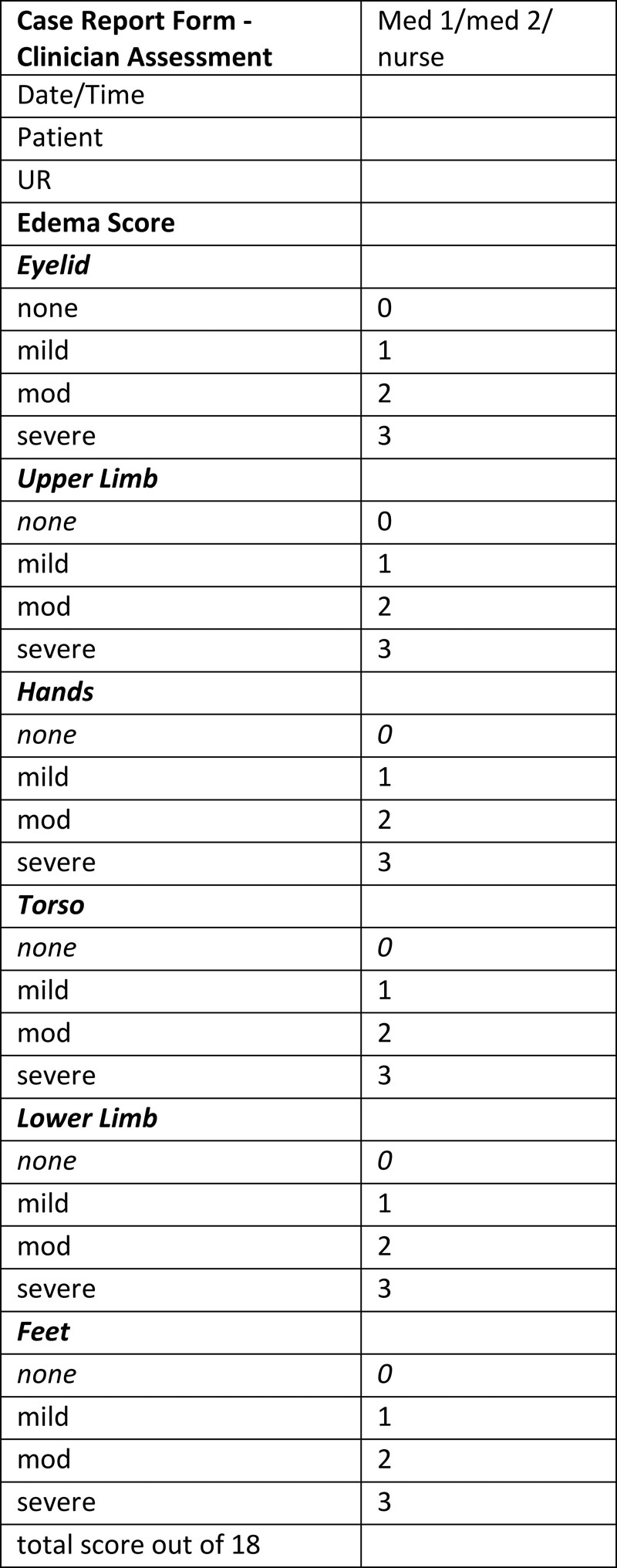
Objectives: To describe a 19-point clinical edema score (CES), investigate its interobserver agreement, and compare changes between such CES and body weight.
Design setting and participants: Prospective observational study in a tertiary PICU of mechanically ventilated children with congenital heart disease.
Main outcomes and measures: Differences in the median CES between observer groups.
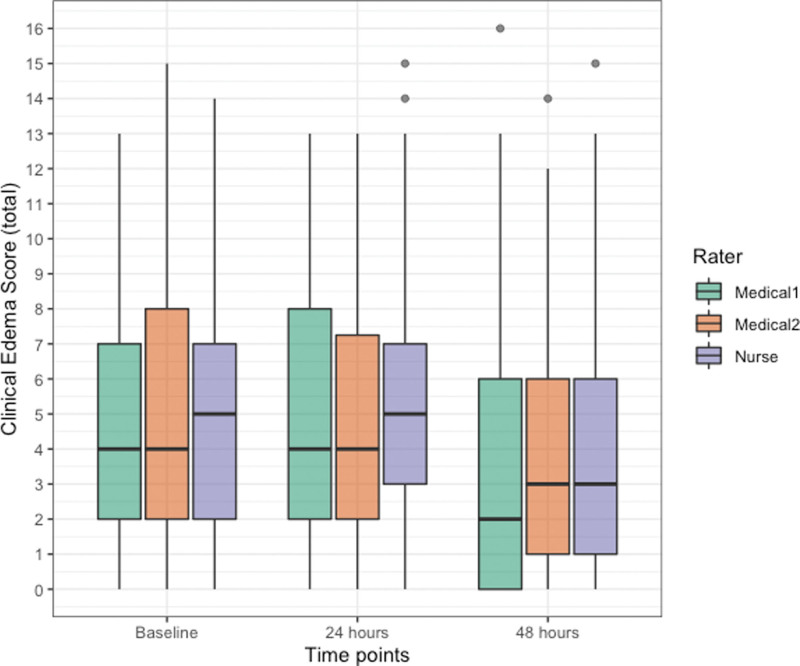
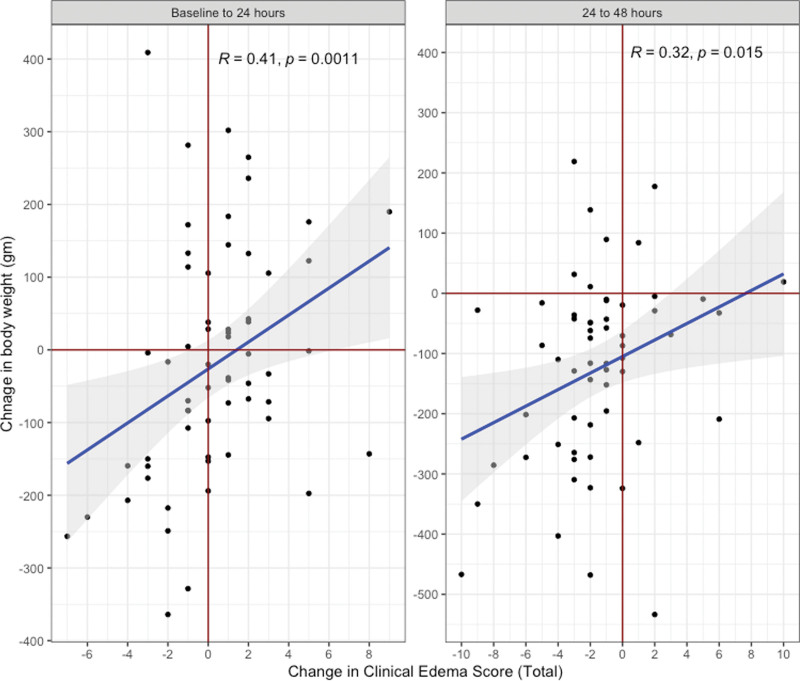
Results: We studied 61 children, with a median age of 8.0 days (interquartile range, 1.0-14.0 d). A total of 539 CES were performed by three observer groups (medical 1 [reference], medical 2, and bedside nurse) at 0, 24, and 48 hours from enrollment. Overall, there was close agreement between observer groups in mean, median, and upper quartile of CES scores, with least agreement observed in the lower quartile of scores. Across all quartiles of CES, after adjusting for baseline weight, cardiac surgical risk, duration of cardiopulmonary bypass, or peritoneal dialysis during the study, observer groups returned similar mean scores (medical 2: 25th centile +0.1 [95% CI, -0.2 to 0.5], median +0.6 [95% CI, -0.4 to 1.5], 75th centile +0.1 [95% CI, -1.1 to 1.4] and nurse: 25th centile +0.5 [95% CI, 0.0-0.9], median +0.7 [95% CI, 0.0-1.5], 75th centile -0.2 [95% CI, -1.3 to 1.0]) Within a multivariable mixed-effects linear regression model, including adjustment for baseline CES, each 1 point increase in CES was associated with a 12.1 grams (95% CI, 3.2-21 grams) increase in body weight.
Conclusions and relevance: In mechanically ventilated children with congenital heart disease, three groups of observers tended to agree when assessing overall edema using an ordinal clinical score assessed in six body regions, with agreement least at low edema scores. An increase in CES was associated with an increase in body weight, suggesting some validity for quantifying edema. Further exploration of the CES as a rapid clinical tool is indicated.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


