{"title":"青少年特发性脊柱侧凸伴胸椎近端主要弯曲的影像学结果。","authors":"Yosuke Horiuchi, Mitsuru Yagi, Satoshi Suzuki, Yohei Takahashi, Satoshi Nori, Osahiko Tsuji, Narihito Nagoshi, Morio Matsumoto, Masaya Nakamura, Kota Watanabe","doi":"10.22603/ssrr.2022-0088","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Adolescent idiopathic scoliosis (AIS) with a major curve at the main thoracic (MT) area is classified as Lenke type 1, 2, or 3 depending on the flexibility of the proximal thoracic (PT) curve and lumbar curve. No definite classification has been established for a major curve at the PT spine. The purpose of this study is to investigate the radiographic characteristics before and after correction surgery for AIS with a major curve at the PT area.</p><p><strong>Methods: </strong>This is a retrospective cohort study at a single academic institution. Twelve patients with a major curve at the PT spine participated in our study and followed for at least two years after surgery. We evaluated the pre- and postoperative Cobb angles of the curve, curve range, location of the apex, sagittal parameters, and shoulder balance-related parameters. All patients were treated by posterior correction and fusion surgery using pedicle screw constructs.</p><p><strong>Results: </strong>The patients were classified as having a double-curve (DC) type, in which the MT curve was structural, or a single-curve (SC) type, in which the MT curve was corrected to less than 25° on supine side-bending films. The mean correction rates for the PT curve were favorable in both groups (DC, 65.7%±9.6%; SC, 39.2%±4.9%). The mean Cobb angle of the lumbar curve improved in the DC group (preoperative, 17.1°±4.0°; postoperative, 5.0°±4.2°) but deteriorated in the SC group (preoperative, 7.1°±1.2°; postoperative, 12.4°±4.4°) after surgery.</p><p><strong>Conclusions: </strong>We illustrated the postoperative radiographical changes of 12 consecutive patients with the major curve at the PT curve. Although posterior correction and fusion surgery corrected the PT curve satisfactorily in both DC and SC patients, the Cobb angle of the lumbar curve deteriorated after surgery in all SC patients. Surgeons need to pay attention to the fusion area, especially LIV, when operating the SC curve type.</p>","PeriodicalId":22253,"journal":{"name":"Spine Surgery and Related Research","volume":"7 4","pages":"371-376"},"PeriodicalIF":1.2000,"publicationDate":"2023-07-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/03/94/2432-261X-7-0371.PMC10447189.pdf","citationCount":"0","resultStr":"{\"title\":\"Radiographical Results of Adolescent Idiopathic Scoliosis with Major Curve at Proximal Thoracic Spine.\",\"authors\":\"Yosuke Horiuchi, Mitsuru Yagi, Satoshi Suzuki, Yohei Takahashi, Satoshi Nori, Osahiko Tsuji, Narihito Nagoshi, Morio Matsumoto, Masaya Nakamura, Kota Watanabe\",\"doi\":\"10.22603/ssrr.2022-0088\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Adolescent idiopathic scoliosis (AIS) with a major curve at the main thoracic (MT) area is classified as Lenke type 1, 2, or 3 depending on the flexibility of the proximal thoracic (PT) curve and lumbar curve. No definite classification has been established for a major curve at the PT spine. The purpose of this study is to investigate the radiographic characteristics before and after correction surgery for AIS with a major curve at the PT area.</p><p><strong>Methods: </strong>This is a retrospective cohort study at a single academic institution. Twelve patients with a major curve at the PT spine participated in our study and followed for at least two years after surgery. We evaluated the pre- and postoperative Cobb angles of the curve, curve range, location of the apex, sagittal parameters, and shoulder balance-related parameters. All patients were treated by posterior correction and fusion surgery using pedicle screw constructs.</p><p><strong>Results: </strong>The patients were classified as having a double-curve (DC) type, in which the MT curve was structural, or a single-curve (SC) type, in which the MT curve was corrected to less than 25° on supine side-bending films. The mean correction rates for the PT curve were favorable in both groups (DC, 65.7%±9.6%; SC, 39.2%±4.9%). The mean Cobb angle of the lumbar curve improved in the DC group (preoperative, 17.1°±4.0°; postoperative, 5.0°±4.2°) but deteriorated in the SC group (preoperative, 7.1°±1.2°; postoperative, 12.4°±4.4°) after surgery.</p><p><strong>Conclusions: </strong>We illustrated the postoperative radiographical changes of 12 consecutive patients with the major curve at the PT curve. Although posterior correction and fusion surgery corrected the PT curve satisfactorily in both DC and SC patients, the Cobb angle of the lumbar curve deteriorated after surgery in all SC patients. Surgeons need to pay attention to the fusion area, especially LIV, when operating the SC curve type.</p>\",\"PeriodicalId\":22253,\"journal\":{\"name\":\"Spine Surgery and Related Research\",\"volume\":\"7 4\",\"pages\":\"371-376\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2023-07-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/03/94/2432-261X-7-0371.PMC10447189.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Spine Surgery and Related Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.22603/ssrr.2022-0088\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Spine Surgery and Related Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22603/ssrr.2022-0088","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
Radiographical Results of Adolescent Idiopathic Scoliosis with Major Curve at Proximal Thoracic Spine.
Introduction: Adolescent idiopathic scoliosis (AIS) with a major curve at the main thoracic (MT) area is classified as Lenke type 1, 2, or 3 depending on the flexibility of the proximal thoracic (PT) curve and lumbar curve. No definite classification has been established for a major curve at the PT spine. The purpose of this study is to investigate the radiographic characteristics before and after correction surgery for AIS with a major curve at the PT area.
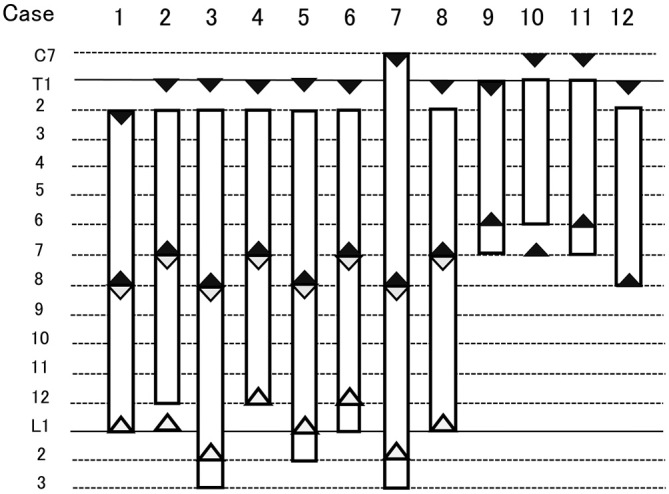
Methods: This is a retrospective cohort study at a single academic institution. Twelve patients with a major curve at the PT spine participated in our study and followed for at least two years after surgery. We evaluated the pre- and postoperative Cobb angles of the curve, curve range, location of the apex, sagittal parameters, and shoulder balance-related parameters. All patients were treated by posterior correction and fusion surgery using pedicle screw constructs.
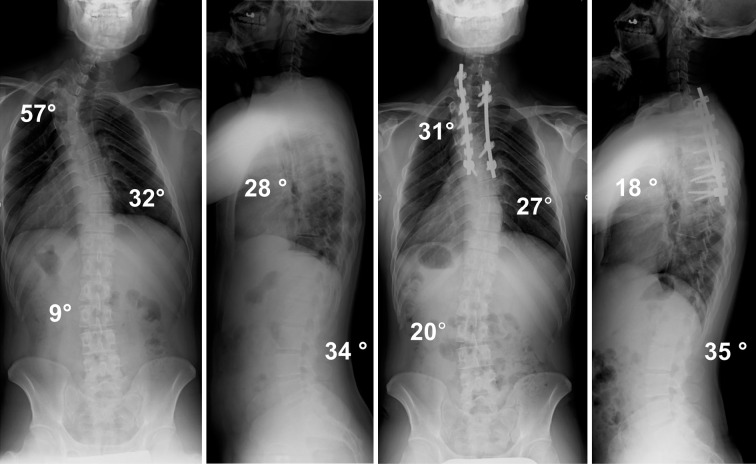
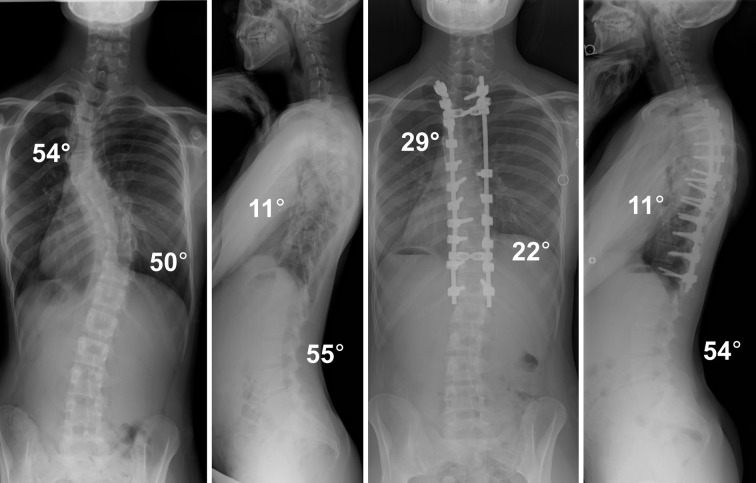
Results: The patients were classified as having a double-curve (DC) type, in which the MT curve was structural, or a single-curve (SC) type, in which the MT curve was corrected to less than 25° on supine side-bending films. The mean correction rates for the PT curve were favorable in both groups (DC, 65.7%±9.6%; SC, 39.2%±4.9%). The mean Cobb angle of the lumbar curve improved in the DC group (preoperative, 17.1°±4.0°; postoperative, 5.0°±4.2°) but deteriorated in the SC group (preoperative, 7.1°±1.2°; postoperative, 12.4°±4.4°) after surgery.
Conclusions: We illustrated the postoperative radiographical changes of 12 consecutive patients with the major curve at the PT curve. Although posterior correction and fusion surgery corrected the PT curve satisfactorily in both DC and SC patients, the Cobb angle of the lumbar curve deteriorated after surgery in all SC patients. Surgeons need to pay attention to the fusion area, especially LIV, when operating the SC curve type.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


