Brooke C D Hockin, Vera-Ellen M Lucci, Ryan E Y Wu, Michelle Nicholas, Iain T Parsons, Victoria E Claydon
{"title":"一项随机对照研究:在没有针刺恐惧症的健康年轻人中,血管内器械操作带来的疼痛会降低正压耐受性并导致血管迷走反应。","authors":"Brooke C D Hockin, Vera-Ellen M Lucci, Ryan E Y Wu, Michelle Nicholas, Iain T Parsons, Victoria E Claydon","doi":"10.1007/s10286-023-00972-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Vasovagal syncope (VVS), or fainting, is frequently triggered by pain, fear, or emotional distress, especially with blood-injection-injury stimuli. We aimed to examine the impact of intravenous (IV) instrumentation on orthostatic tolerance (OT; fainting susceptibility) in healthy young adults. We hypothesized that pain associated with IV procedures would reduce OT.</p><p><strong>Methods: </strong>In this randomised, double-blind, placebo-controlled, cross-over study, participants (N = 23; 14 women; age 24.2 ± 4.4 years) underwent head-up tilt with combined lower body negative pressure to presyncope on three separate days: (1) IV cannulation with local anaesthetic cream (EMLA) (IV + EMLA); (2) IV cannulation with placebo cream (IV + Placebo); (3) sham IV cannulation with local anaesthetic cream (Sham + EMLA). Participants rated pain associated with IV procedures on a 1-5 scale. Cardiovascular (finger plethysmography and electrocardiogram; Finometer Pro), and forearm vascular resistance (FVR; brachial Doppler) responses were recorded continuously and non-invasively.</p><p><strong>Results: </strong>Compared to Sham + EMLA (27.8 ± 2.4 min), OT was reduced in IV + Placebo (23.0 ± 2.8 min; p = 0.026), but not in IV + EMLA (26.2 ± 2.2 min; p = 0.185). Pain was increased in IV + Placebo (2.8 ± 0.2) compared to IV + EMLA (2.0 ± 2.2; p = 0.002) and Sham + EMLA (1.1 ± 0.1; p < 0.001). Orthostatic heart rate responses were lower in IV + Placebo (84.4 ± 3.1 bpm) than IV + EMLA (87.3 ± 3.1 bpm; p = 0.007) and Sham + EMLA (87.7 ± 3.1 bpm; p = 0.001). Maximal FVR responses were reduced in IV + Placebo (+ 140.7 ± 19.0%) compared to IV + EMLA (+ 221.2 ± 25.9%; p < 0.001) and Sham + EMLA (+ 190.6 ± 17.0%; p = 0.017).</p><p><strong>Conclusions: </strong>Pain plays a key role in predisposing to VVS following venipuncture, and our data suggest this effect is mediated through reduced capacity to achieve maximal sympathetic activation during orthostatic stress. Topical anaesthetics, such as EMLA, may reduce the frequency and severity of VVS during procedures requiring needles and intravascular instrumentation.</p>","PeriodicalId":10168,"journal":{"name":"Clinical Autonomic Research","volume":" ","pages":"673-689"},"PeriodicalIF":3.9000,"publicationDate":"2023-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Pain associated with intravascular instrumentation reduces orthostatic tolerance and predisposes to vasovagal reactions in healthy young adults without needle phobia: a randomised controlled study.\",\"authors\":\"Brooke C D Hockin, Vera-Ellen M Lucci, Ryan E Y Wu, Michelle Nicholas, Iain T Parsons, Victoria E Claydon\",\"doi\":\"10.1007/s10286-023-00972-8\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Vasovagal syncope (VVS), or fainting, is frequently triggered by pain, fear, or emotional distress, especially with blood-injection-injury stimuli. We aimed to examine the impact of intravenous (IV) instrumentation on orthostatic tolerance (OT; fainting susceptibility) in healthy young adults. We hypothesized that pain associated with IV procedures would reduce OT.</p><p><strong>Methods: </strong>In this randomised, double-blind, placebo-controlled, cross-over study, participants (N = 23; 14 women; age 24.2 ± 4.4 years) underwent head-up tilt with combined lower body negative pressure to presyncope on three separate days: (1) IV cannulation with local anaesthetic cream (EMLA) (IV + EMLA); (2) IV cannulation with placebo cream (IV + Placebo); (3) sham IV cannulation with local anaesthetic cream (Sham + EMLA). Participants rated pain associated with IV procedures on a 1-5 scale. Cardiovascular (finger plethysmography and electrocardiogram; Finometer Pro), and forearm vascular resistance (FVR; brachial Doppler) responses were recorded continuously and non-invasively.</p><p><strong>Results: </strong>Compared to Sham + EMLA (27.8 ± 2.4 min), OT was reduced in IV + Placebo (23.0 ± 2.8 min; p = 0.026), but not in IV + EMLA (26.2 ± 2.2 min; p = 0.185). Pain was increased in IV + Placebo (2.8 ± 0.2) compared to IV + EMLA (2.0 ± 2.2; p = 0.002) and Sham + EMLA (1.1 ± 0.1; p < 0.001). Orthostatic heart rate responses were lower in IV + Placebo (84.4 ± 3.1 bpm) than IV + EMLA (87.3 ± 3.1 bpm; p = 0.007) and Sham + EMLA (87.7 ± 3.1 bpm; p = 0.001). Maximal FVR responses were reduced in IV + Placebo (+ 140.7 ± 19.0%) compared to IV + EMLA (+ 221.2 ± 25.9%; p < 0.001) and Sham + EMLA (+ 190.6 ± 17.0%; p = 0.017).</p><p><strong>Conclusions: </strong>Pain plays a key role in predisposing to VVS following venipuncture, and our data suggest this effect is mediated through reduced capacity to achieve maximal sympathetic activation during orthostatic stress. Topical anaesthetics, such as EMLA, may reduce the frequency and severity of VVS during procedures requiring needles and intravascular instrumentation.</p>\",\"PeriodicalId\":10168,\"journal\":{\"name\":\"Clinical Autonomic Research\",\"volume\":\" \",\"pages\":\"673-689\"},\"PeriodicalIF\":3.9000,\"publicationDate\":\"2023-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Autonomic Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s10286-023-00972-8\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/8/17 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Autonomic Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10286-023-00972-8","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/8/17 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Pain associated with intravascular instrumentation reduces orthostatic tolerance and predisposes to vasovagal reactions in healthy young adults without needle phobia: a randomised controlled study.
Purpose: Vasovagal syncope (VVS), or fainting, is frequently triggered by pain, fear, or emotional distress, especially with blood-injection-injury stimuli. We aimed to examine the impact of intravenous (IV) instrumentation on orthostatic tolerance (OT; fainting susceptibility) in healthy young adults. We hypothesized that pain associated with IV procedures would reduce OT.
Methods: In this randomised, double-blind, placebo-controlled, cross-over study, participants (N = 23; 14 women; age 24.2 ± 4.4 years) underwent head-up tilt with combined lower body negative pressure to presyncope on three separate days: (1) IV cannulation with local anaesthetic cream (EMLA) (IV + EMLA); (2) IV cannulation with placebo cream (IV + Placebo); (3) sham IV cannulation with local anaesthetic cream (Sham + EMLA). Participants rated pain associated with IV procedures on a 1-5 scale. Cardiovascular (finger plethysmography and electrocardiogram; Finometer Pro), and forearm vascular resistance (FVR; brachial Doppler) responses were recorded continuously and non-invasively.
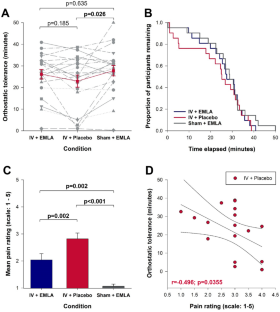
Results: Compared to Sham + EMLA (27.8 ± 2.4 min), OT was reduced in IV + Placebo (23.0 ± 2.8 min; p = 0.026), but not in IV + EMLA (26.2 ± 2.2 min; p = 0.185). Pain was increased in IV + Placebo (2.8 ± 0.2) compared to IV + EMLA (2.0 ± 2.2; p = 0.002) and Sham + EMLA (1.1 ± 0.1; p < 0.001). Orthostatic heart rate responses were lower in IV + Placebo (84.4 ± 3.1 bpm) than IV + EMLA (87.3 ± 3.1 bpm; p = 0.007) and Sham + EMLA (87.7 ± 3.1 bpm; p = 0.001). Maximal FVR responses were reduced in IV + Placebo (+ 140.7 ± 19.0%) compared to IV + EMLA (+ 221.2 ± 25.9%; p < 0.001) and Sham + EMLA (+ 190.6 ± 17.0%; p = 0.017).
Conclusions: Pain plays a key role in predisposing to VVS following venipuncture, and our data suggest this effect is mediated through reduced capacity to achieve maximal sympathetic activation during orthostatic stress. Topical anaesthetics, such as EMLA, may reduce the frequency and severity of VVS during procedures requiring needles and intravascular instrumentation.
期刊介绍:
Clinical Autonomic Research aims to draw together and disseminate research work from various disciplines and specialties dealing with clinical problems resulting from autonomic dysfunction. Areas to be covered include: cardiovascular system, neurology, diabetes, endocrinology, urology, pain disorders, ophthalmology, gastroenterology, toxicology and clinical pharmacology, skin infectious diseases, renal disease.
This journal is an essential source of new information for everyone working in areas involving the autonomic nervous system. A major feature of Clinical Autonomic Research is its speed of publication coupled with the highest refereeing standards.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


