Hernando Gómez, Alexander Zarbock, Stephen M Pastores, Gyorgy Frendl, Sven Bercker, Pierre Asfar, Steven A Conrad, Jaques Creteur, James Miner, Jean Paul Mira, Johan Motsch, Jean-Pierre Quenot, Thomas Rimmelé, Peter Rosenberger, Christophe Vinsonneau, Bob Birch, Fabienne Heskia, Julien Textoris, Luca Molinari, Louis M Guzzi, Claudio Ronco, John A Kellum
{"title":"生物标志物引导的保肾脓毒症治疗束的可行性评估:脓毒症试验中限制急性肾损伤进展。","authors":"Hernando Gómez, Alexander Zarbock, Stephen M Pastores, Gyorgy Frendl, Sven Bercker, Pierre Asfar, Steven A Conrad, Jaques Creteur, James Miner, Jean Paul Mira, Johan Motsch, Jean-Pierre Quenot, Thomas Rimmelé, Peter Rosenberger, Christophe Vinsonneau, Bob Birch, Fabienne Heskia, Julien Textoris, Luca Molinari, Louis M Guzzi, Claudio Ronco, John A Kellum","doi":"10.1097/CCE.0000000000000961","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To determine the feasibility, safety, and efficacy of a biomarker-guided implementation of a kidney-sparing sepsis bundle (KSSB) of care in comparison with standard of care (SOC) on clinical outcomes in patients with sepsis.</p><p><strong>Design: </strong>Adaptive, multicenter, randomized clinical trial.</p><p><strong>Setting: </strong>Five University Hospitals in Europe and North America.</p><p><strong>Patients: </strong>Adult patients, admitted to the ICU with an indwelling urinary catheter and diagnosis of sepsis or septic shock, without acute kidney injury (acute kidney injury) stage 2 or 3 or chronic kidney disease.</p><p><strong>Interventions: </strong>A three-level KSSB based on Kidney Disease: Improving Global Outcomes (KDIGOs) recommendations guided by serial measurements of urinary tissue inhibitor of metalloproteinases-2 and insulin-like growth factor-binding protein 7 used as a combined biomarker [TIMP2]•[IGFBP7].</p><p><strong>Measurements and main results: </strong>The trial was stopped for low enrollment related to the COVID-19 pandemic. Nineteen patients enrolled in five sites over 12 months were randomized to the SOC (<i>n</i> = 8, 42.0%) or intervention (<i>n</i> = 11, 58.0%). The primary outcome was feasibility, and key secondary outcomes were safety and efficacy. Adherence to protocol in patients assigned to the first two levels of KSSB was 15 of 19 (81.8%) and 19 of 19 (100%) but was 1 of 4 (25%) for level 3 KSSB. Serious adverse events were more frequent in the intervention arm (4/11, 36.4%) than in the control arm (1/8, 12.5%), but none were related to study interventions. The secondary efficacy outcome was a composite of death, dialysis, or progression of greater than or equal to 2 stages of acute kidney injury within 72 hours after enrollment and was reached by 3 of 8 (37.5%) patients in the control arm, and 0 of 11 (0%) patients in the intervention arm. In the control arm, two patients experienced progression of acute kidney injury, and one patient died.</p><p><strong>Conclusions: </strong>Although the COVID-19 pandemic impeded recruitment, the actual implementation of a therapeutic strategy that deploys a KDIGO-based KSSB of care guided by risk stratification using urinary [TIMP2]•[IGFBP7] seems feasible and appears to be safe in patients with sepsis.</p>","PeriodicalId":10759,"journal":{"name":"Critical Care Explorations","volume":"5 8","pages":"e0961"},"PeriodicalIF":0.0000,"publicationDate":"2023-08-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/0f/3f/cc9-5-e0961.PMC10443738.pdf","citationCount":"0","resultStr":"{\"title\":\"Feasibility Assessment of a Biomarker-Guided Kidney-Sparing Sepsis Bundle: The Limiting Acute Kidney Injury Progression In Sepsis Trial.\",\"authors\":\"Hernando Gómez, Alexander Zarbock, Stephen M Pastores, Gyorgy Frendl, Sven Bercker, Pierre Asfar, Steven A Conrad, Jaques Creteur, James Miner, Jean Paul Mira, Johan Motsch, Jean-Pierre Quenot, Thomas Rimmelé, Peter Rosenberger, Christophe Vinsonneau, Bob Birch, Fabienne Heskia, Julien Textoris, Luca Molinari, Louis M Guzzi, Claudio Ronco, John A Kellum\",\"doi\":\"10.1097/CCE.0000000000000961\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>To determine the feasibility, safety, and efficacy of a biomarker-guided implementation of a kidney-sparing sepsis bundle (KSSB) of care in comparison with standard of care (SOC) on clinical outcomes in patients with sepsis.</p><p><strong>Design: </strong>Adaptive, multicenter, randomized clinical trial.</p><p><strong>Setting: </strong>Five University Hospitals in Europe and North America.</p><p><strong>Patients: </strong>Adult patients, admitted to the ICU with an indwelling urinary catheter and diagnosis of sepsis or septic shock, without acute kidney injury (acute kidney injury) stage 2 or 3 or chronic kidney disease.</p><p><strong>Interventions: </strong>A three-level KSSB based on Kidney Disease: Improving Global Outcomes (KDIGOs) recommendations guided by serial measurements of urinary tissue inhibitor of metalloproteinases-2 and insulin-like growth factor-binding protein 7 used as a combined biomarker [TIMP2]•[IGFBP7].</p><p><strong>Measurements and main results: </strong>The trial was stopped for low enrollment related to the COVID-19 pandemic. Nineteen patients enrolled in five sites over 12 months were randomized to the SOC (<i>n</i> = 8, 42.0%) or intervention (<i>n</i> = 11, 58.0%). The primary outcome was feasibility, and key secondary outcomes were safety and efficacy. Adherence to protocol in patients assigned to the first two levels of KSSB was 15 of 19 (81.8%) and 19 of 19 (100%) but was 1 of 4 (25%) for level 3 KSSB. Serious adverse events were more frequent in the intervention arm (4/11, 36.4%) than in the control arm (1/8, 12.5%), but none were related to study interventions. The secondary efficacy outcome was a composite of death, dialysis, or progression of greater than or equal to 2 stages of acute kidney injury within 72 hours after enrollment and was reached by 3 of 8 (37.5%) patients in the control arm, and 0 of 11 (0%) patients in the intervention arm. In the control arm, two patients experienced progression of acute kidney injury, and one patient died.</p><p><strong>Conclusions: </strong>Although the COVID-19 pandemic impeded recruitment, the actual implementation of a therapeutic strategy that deploys a KDIGO-based KSSB of care guided by risk stratification using urinary [TIMP2]•[IGFBP7] seems feasible and appears to be safe in patients with sepsis.</p>\",\"PeriodicalId\":10759,\"journal\":{\"name\":\"Critical Care Explorations\",\"volume\":\"5 8\",\"pages\":\"e0961\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-08-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/0f/3f/cc9-5-e0961.PMC10443738.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical Care Explorations\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/CCE.0000000000000961\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/8/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Care Explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000000961","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/8/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Feasibility Assessment of a Biomarker-Guided Kidney-Sparing Sepsis Bundle: The Limiting Acute Kidney Injury Progression In Sepsis Trial.
Objectives: To determine the feasibility, safety, and efficacy of a biomarker-guided implementation of a kidney-sparing sepsis bundle (KSSB) of care in comparison with standard of care (SOC) on clinical outcomes in patients with sepsis.
Setting: Five University Hospitals in Europe and North America.
Patients: Adult patients, admitted to the ICU with an indwelling urinary catheter and diagnosis of sepsis or septic shock, without acute kidney injury (acute kidney injury) stage 2 or 3 or chronic kidney disease.
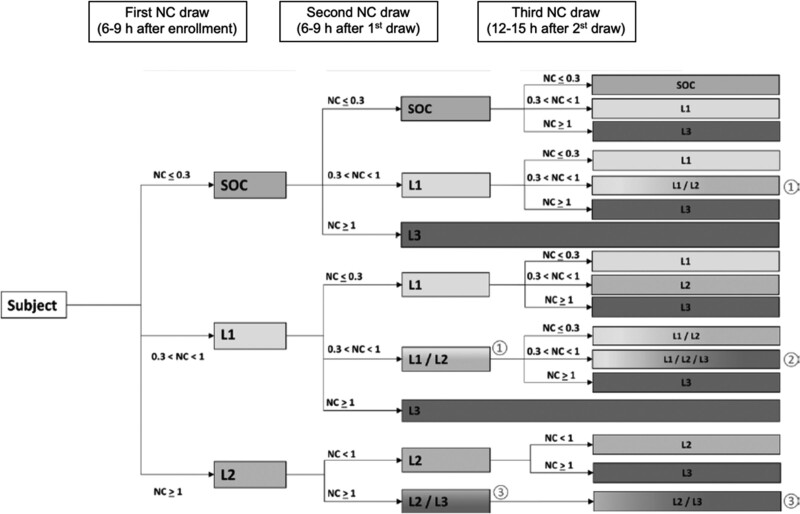
Interventions: A three-level KSSB based on Kidney Disease: Improving Global Outcomes (KDIGOs) recommendations guided by serial measurements of urinary tissue inhibitor of metalloproteinases-2 and insulin-like growth factor-binding protein 7 used as a combined biomarker [TIMP2]•[IGFBP7].
Measurements and main results: The trial was stopped for low enrollment related to the COVID-19 pandemic. Nineteen patients enrolled in five sites over 12 months were randomized to the SOC (n = 8, 42.0%) or intervention (n = 11, 58.0%). The primary outcome was feasibility, and key secondary outcomes were safety and efficacy. Adherence to protocol in patients assigned to the first two levels of KSSB was 15 of 19 (81.8%) and 19 of 19 (100%) but was 1 of 4 (25%) for level 3 KSSB. Serious adverse events were more frequent in the intervention arm (4/11, 36.4%) than in the control arm (1/8, 12.5%), but none were related to study interventions. The secondary efficacy outcome was a composite of death, dialysis, or progression of greater than or equal to 2 stages of acute kidney injury within 72 hours after enrollment and was reached by 3 of 8 (37.5%) patients in the control arm, and 0 of 11 (0%) patients in the intervention arm. In the control arm, two patients experienced progression of acute kidney injury, and one patient died.
Conclusions: Although the COVID-19 pandemic impeded recruitment, the actual implementation of a therapeutic strategy that deploys a KDIGO-based KSSB of care guided by risk stratification using urinary [TIMP2]•[IGFBP7] seems feasible and appears to be safe in patients with sepsis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


