{"title":"腹腔镜胰十二指肠切除术和腹腔镜胰十二指肠切除术与机器人重建:单个外科医生的经验和技术注意事项。","authors":"Jae Young Jang, Eui Hyuk Chong, Incheon Kang, Seok Jeon Yang, Sung Hwan Lee, Sung Hoon Choi","doi":"10.7602/jmis.2023.26.2.72","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Despite the increasing number of robotic pancreaticoduodenectomies, laparoscopic pancreaticoduodenectomy (LPD) and LPD with robotic reconstruction (LPD-RR) are still valuable surgical options for minimally invasive pancreaticoduodenectomy (MIPD). This study introduces the surgical techniques, tips, and outcomes of our experience with LPD and LPD-RR.</p><p><strong>Methods: </strong>Between March 2014 and July 2021, 122 and 48 patients underwent LPD and LPD-RR respectively, at CHA Bundang Medical Center in Korea. The operative settings, procedures, and trocar placements were identical in both approaches; however, different trocars were used. We introduced our techniques of retraction methods for Kocherization and uncinate process dissection, pancreatic reconstruction, pancreatic division, and protection using the round ligament. The perioperative surgical outcomes of LPD and LPD-RR were compared.</p><p><strong>Results: </strong>Baseline demographics of patients in the LPD and LPD-RR groups were comparable, but the LPD group had older age (65.5 ± 11.6 years vs. 60.0 ± 14.1 years, <i>p</i> = 0.009) and lesser preoperative chemotherapy (15.6% vs. 35.4%, <i>p</i> = 0.008). The proportion of malignant disease was similar (LPD group, 86.1% vs. LPD-RR group, 83.3%; <i>p</i> = 0.759). Perioperative outcomes were also comparable, including operative time, estimated blood loss, clinically relevant postoperative pancreatic fistula (LPD group, 9.0% vs. LPD-RR group, 10.4%; <i>p</i> = 0.684), and major postoperative complication rates (LPD group, 14.8% vs. LPD-RR group, 6.2%; <i>p</i> = 0.082).</p><p><strong>Conclusion: </strong>Both LPD and LPR-RR can be safely performed by experienced surgeons with acceptable surgical outcomes. Further investigations are required to evaluate the objective benefits of robotic surgical systems in MIPD and establish widely acceptable standardized MIPD techniques.</p>","PeriodicalId":73832,"journal":{"name":"Journal of minimally invasive surgery","volume":"26 2","pages":"72-82"},"PeriodicalIF":0.0000,"publicationDate":"2023-06-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c3/e9/jmis-26-2-72.PMC10280110.pdf","citationCount":"1","resultStr":"{\"title\":\"Laparoscopic pancreaticoduodenectomy and laparoscopic pancreaticoduodenectomy with robotic reconstruction: single-surgeon experience and technical notes.\",\"authors\":\"Jae Young Jang, Eui Hyuk Chong, Incheon Kang, Seok Jeon Yang, Sung Hwan Lee, Sung Hoon Choi\",\"doi\":\"10.7602/jmis.2023.26.2.72\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Despite the increasing number of robotic pancreaticoduodenectomies, laparoscopic pancreaticoduodenectomy (LPD) and LPD with robotic reconstruction (LPD-RR) are still valuable surgical options for minimally invasive pancreaticoduodenectomy (MIPD). This study introduces the surgical techniques, tips, and outcomes of our experience with LPD and LPD-RR.</p><p><strong>Methods: </strong>Between March 2014 and July 2021, 122 and 48 patients underwent LPD and LPD-RR respectively, at CHA Bundang Medical Center in Korea. The operative settings, procedures, and trocar placements were identical in both approaches; however, different trocars were used. We introduced our techniques of retraction methods for Kocherization and uncinate process dissection, pancreatic reconstruction, pancreatic division, and protection using the round ligament. The perioperative surgical outcomes of LPD and LPD-RR were compared.</p><p><strong>Results: </strong>Baseline demographics of patients in the LPD and LPD-RR groups were comparable, but the LPD group had older age (65.5 ± 11.6 years vs. 60.0 ± 14.1 years, <i>p</i> = 0.009) and lesser preoperative chemotherapy (15.6% vs. 35.4%, <i>p</i> = 0.008). The proportion of malignant disease was similar (LPD group, 86.1% vs. LPD-RR group, 83.3%; <i>p</i> = 0.759). Perioperative outcomes were also comparable, including operative time, estimated blood loss, clinically relevant postoperative pancreatic fistula (LPD group, 9.0% vs. LPD-RR group, 10.4%; <i>p</i> = 0.684), and major postoperative complication rates (LPD group, 14.8% vs. LPD-RR group, 6.2%; <i>p</i> = 0.082).</p><p><strong>Conclusion: </strong>Both LPD and LPR-RR can be safely performed by experienced surgeons with acceptable surgical outcomes. Further investigations are required to evaluate the objective benefits of robotic surgical systems in MIPD and establish widely acceptable standardized MIPD techniques.</p>\",\"PeriodicalId\":73832,\"journal\":{\"name\":\"Journal of minimally invasive surgery\",\"volume\":\"26 2\",\"pages\":\"72-82\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-06-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c3/e9/jmis-26-2-72.PMC10280110.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of minimally invasive surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.7602/jmis.2023.26.2.72\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of minimally invasive surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.7602/jmis.2023.26.2.72","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Laparoscopic pancreaticoduodenectomy and laparoscopic pancreaticoduodenectomy with robotic reconstruction: single-surgeon experience and technical notes.
Purpose: Despite the increasing number of robotic pancreaticoduodenectomies, laparoscopic pancreaticoduodenectomy (LPD) and LPD with robotic reconstruction (LPD-RR) are still valuable surgical options for minimally invasive pancreaticoduodenectomy (MIPD). This study introduces the surgical techniques, tips, and outcomes of our experience with LPD and LPD-RR.
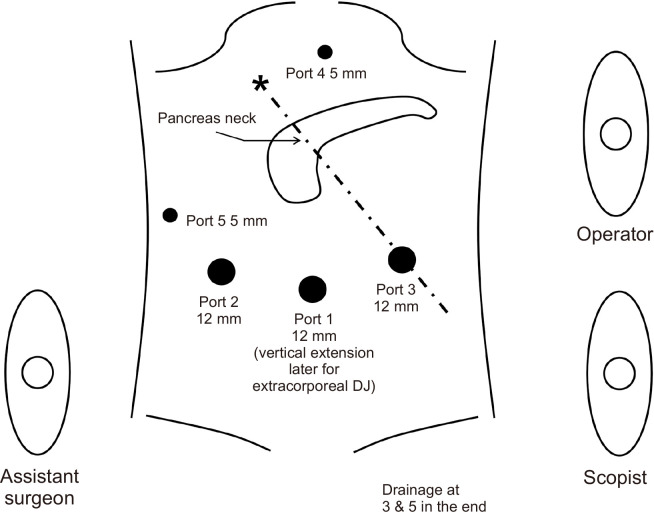
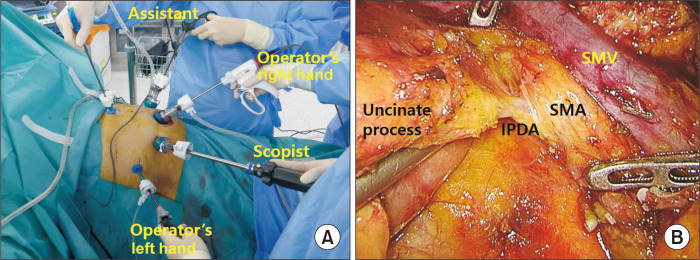
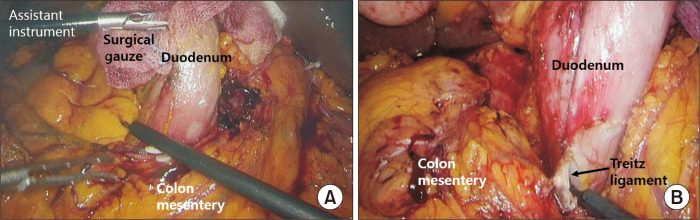
Methods: Between March 2014 and July 2021, 122 and 48 patients underwent LPD and LPD-RR respectively, at CHA Bundang Medical Center in Korea. The operative settings, procedures, and trocar placements were identical in both approaches; however, different trocars were used. We introduced our techniques of retraction methods for Kocherization and uncinate process dissection, pancreatic reconstruction, pancreatic division, and protection using the round ligament. The perioperative surgical outcomes of LPD and LPD-RR were compared.
Results: Baseline demographics of patients in the LPD and LPD-RR groups were comparable, but the LPD group had older age (65.5 ± 11.6 years vs. 60.0 ± 14.1 years, p = 0.009) and lesser preoperative chemotherapy (15.6% vs. 35.4%, p = 0.008). The proportion of malignant disease was similar (LPD group, 86.1% vs. LPD-RR group, 83.3%; p = 0.759). Perioperative outcomes were also comparable, including operative time, estimated blood loss, clinically relevant postoperative pancreatic fistula (LPD group, 9.0% vs. LPD-RR group, 10.4%; p = 0.684), and major postoperative complication rates (LPD group, 14.8% vs. LPD-RR group, 6.2%; p = 0.082).
Conclusion: Both LPD and LPR-RR can be safely performed by experienced surgeons with acceptable surgical outcomes. Further investigations are required to evaluate the objective benefits of robotic surgical systems in MIPD and establish widely acceptable standardized MIPD techniques.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


