Maya Satheeskaran, Aminah Hussan, Ailin Anto, Laure de Preux
{"title":"抗生素预防与非抗生素预防急性胆囊切除术的成本-效果分析。","authors":"Maya Satheeskaran, Aminah Hussan, Ailin Anto, Laure de Preux","doi":"10.1136/bmjgast-2023-001162","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>For acute cholecystitis, the treatment of choice is laparoscopic cholecystectomy. In mild-to-moderate cases, the use of antibiotic prophylaxis for the prevention of postoperative infectious complications (POICs) lacks evidence regarding its cost-effectiveness when compared with no prophylaxis. In the context of rising antimicrobial resistance, there is a clear rationale for a cost-effectiveness analysis (CEA) to determine the most efficient use of National Health Service resources and antibiotic routine usage.</p><p><strong>Design: </strong>16 of 226 patients (7.1%) in the single-dose prophylaxis group and 29 of 231 (12.6%) in the non-prophylaxis group developed POICs. A CEA was carried out using health outcome data from thePerioperative antibiotic prophylaxis in the treatment of acute cholecystitis (PEANUTS II) multicentre, randomised, open-label, non-inferiority, clinical trial. Costs were measured in monetary units using pound sterling, and effectiveness expressed as POICs avoided within the first 30 days after cholecystectomy.</p><p><strong>Results: </strong>This CEA produced an incremental cost-effectiveness ratio of -£792.70. This suggests a modest cost-effectiveness of antibiotic prophylaxis being marginally less costly and more effective than no prophylaxis. Three sensitivity analyses were executed considering full adherence to the antibiotic, POICs with increased complexity and break-point analysis suggesting caution in the recommendation of systematic use of antibiotic prophylaxis for the prevention of POICs.</p><p><strong>Conclusion: </strong>The results of this CEA point to greater consensus in UK-based guidelines surrounding the provision of antibiotic prophylaxis for mild-to-moderate cases of acute cholecystitis.</p>","PeriodicalId":9235,"journal":{"name":"BMJ Open Gastroenterology","volume":"10 1","pages":""},"PeriodicalIF":3.3000,"publicationDate":"2023-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d4/cd/bmjgast-2023-001162.PMC10423775.pdf","citationCount":"0","resultStr":"{\"title\":\"Cost-effectiveness analysis of antibiotic prophylaxis versus no antibiotic prophylaxis for acute cholecystectomy.\",\"authors\":\"Maya Satheeskaran, Aminah Hussan, Ailin Anto, Laure de Preux\",\"doi\":\"10.1136/bmjgast-2023-001162\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>For acute cholecystitis, the treatment of choice is laparoscopic cholecystectomy. In mild-to-moderate cases, the use of antibiotic prophylaxis for the prevention of postoperative infectious complications (POICs) lacks evidence regarding its cost-effectiveness when compared with no prophylaxis. In the context of rising antimicrobial resistance, there is a clear rationale for a cost-effectiveness analysis (CEA) to determine the most efficient use of National Health Service resources and antibiotic routine usage.</p><p><strong>Design: </strong>16 of 226 patients (7.1%) in the single-dose prophylaxis group and 29 of 231 (12.6%) in the non-prophylaxis group developed POICs. A CEA was carried out using health outcome data from thePerioperative antibiotic prophylaxis in the treatment of acute cholecystitis (PEANUTS II) multicentre, randomised, open-label, non-inferiority, clinical trial. Costs were measured in monetary units using pound sterling, and effectiveness expressed as POICs avoided within the first 30 days after cholecystectomy.</p><p><strong>Results: </strong>This CEA produced an incremental cost-effectiveness ratio of -£792.70. This suggests a modest cost-effectiveness of antibiotic prophylaxis being marginally less costly and more effective than no prophylaxis. Three sensitivity analyses were executed considering full adherence to the antibiotic, POICs with increased complexity and break-point analysis suggesting caution in the recommendation of systematic use of antibiotic prophylaxis for the prevention of POICs.</p><p><strong>Conclusion: </strong>The results of this CEA point to greater consensus in UK-based guidelines surrounding the provision of antibiotic prophylaxis for mild-to-moderate cases of acute cholecystitis.</p>\",\"PeriodicalId\":9235,\"journal\":{\"name\":\"BMJ Open Gastroenterology\",\"volume\":\"10 1\",\"pages\":\"\"},\"PeriodicalIF\":3.3000,\"publicationDate\":\"2023-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d4/cd/bmjgast-2023-001162.PMC10423775.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ Open Gastroenterology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjgast-2023-001162\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Open Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjgast-2023-001162","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Cost-effectiveness analysis of antibiotic prophylaxis versus no antibiotic prophylaxis for acute cholecystectomy.
Objective: For acute cholecystitis, the treatment of choice is laparoscopic cholecystectomy. In mild-to-moderate cases, the use of antibiotic prophylaxis for the prevention of postoperative infectious complications (POICs) lacks evidence regarding its cost-effectiveness when compared with no prophylaxis. In the context of rising antimicrobial resistance, there is a clear rationale for a cost-effectiveness analysis (CEA) to determine the most efficient use of National Health Service resources and antibiotic routine usage.
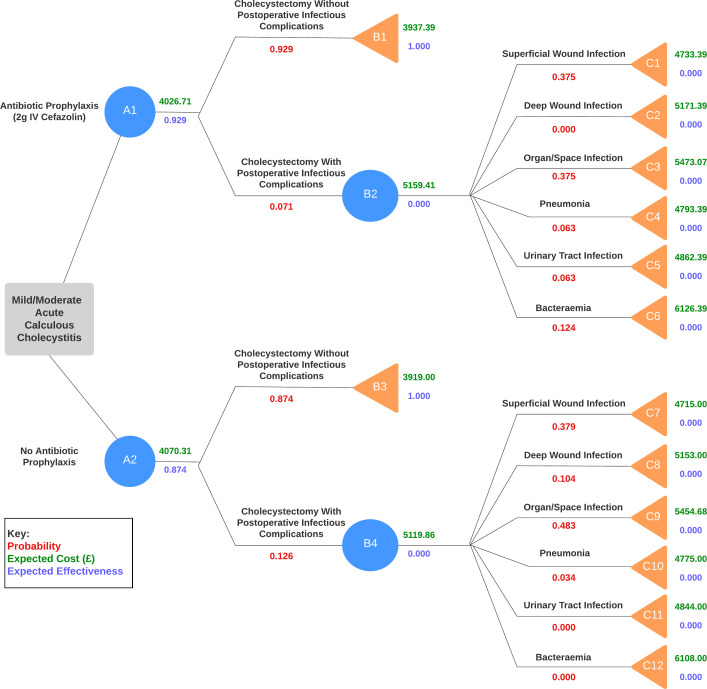
Design: 16 of 226 patients (7.1%) in the single-dose prophylaxis group and 29 of 231 (12.6%) in the non-prophylaxis group developed POICs. A CEA was carried out using health outcome data from thePerioperative antibiotic prophylaxis in the treatment of acute cholecystitis (PEANUTS II) multicentre, randomised, open-label, non-inferiority, clinical trial. Costs were measured in monetary units using pound sterling, and effectiveness expressed as POICs avoided within the first 30 days after cholecystectomy.
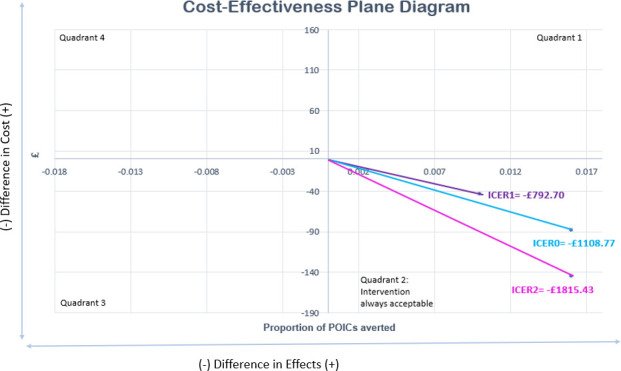
Results: This CEA produced an incremental cost-effectiveness ratio of -£792.70. This suggests a modest cost-effectiveness of antibiotic prophylaxis being marginally less costly and more effective than no prophylaxis. Three sensitivity analyses were executed considering full adherence to the antibiotic, POICs with increased complexity and break-point analysis suggesting caution in the recommendation of systematic use of antibiotic prophylaxis for the prevention of POICs.
Conclusion: The results of this CEA point to greater consensus in UK-based guidelines surrounding the provision of antibiotic prophylaxis for mild-to-moderate cases of acute cholecystitis.
期刊介绍:
BMJ Open Gastroenterology is an online-only, peer-reviewed, open access gastroenterology journal, dedicated to publishing high-quality medical research from all disciplines and therapeutic areas of gastroenterology. It is the open access companion journal of Gut and is co-owned by the British Society of Gastroenterology. The journal publishes all research study types, from study protocols to phase I trials to meta-analyses, including small or specialist studies. Publishing procedures are built around continuous publication, publishing research online as soon as the article is ready.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


