{"title":"Budd-Chiari综合征作为系统性红斑狼疮伴抗磷脂综合征的初始表现:1例报告并文献复习。","authors":"Gashaw Solela, Merga Daba","doi":"10.2147/OARRR.S425535","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Budd-Chiari syndrome (BCS) is a rare disorder characterized by hepatic outflow obstruction. It can be classified as primary or secondary BCS. Common causes of BCS include myeloproliferative diseases, infections, malignancies, and systemic autoimmune illnesses. Systemic lupus erythematosus (SLE) can be complicated with BCS. However, only a few case reports have described the uncommon occurrence of BCS as a primary presentation of SLE.</p><p><strong>Case presentation: </strong>We report the case of a 32-year-old female patient who presented with progressive abdominal distension of four months. On the abdominal CT scan, the left and middle hepatic veins were not visualized; the right hepatic vein and intrahepatic IVC had luminal narrowing; and there was caudate lobe enlargement suggestive of Budd-Chiari syndrome (BCS). Six months after the diagnosis of BCS, the patient developed other clinical features suggestive of systemic lupus erythematosus (SLE) and was finally diagnosed with SLE.</p><p><strong>Conclusion: </strong>Acquired or inherited thrombotic conditions are the most common underlying causes of Budd-Chiari syndrome. Systemic lupus erythematosus (SLE) is the most common cause of secondary APS and most patients present with Budd-Chiari syndrome as a manifestation of APS after the diagnosis of SLE. In rare cases, such as the current case, Budd-Chiari syndrome can present even before the diagnosis of SLE. Hence, we would like to emphasize that Budd-Chiari syndrome can be an initial presentation of SLE.</p>","PeriodicalId":45545,"journal":{"name":"Open Access Rheumatology-Research and Reviews","volume":"15 ","pages":"139-143"},"PeriodicalIF":1.7000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/06/1b/oarrr-15-139.PMC10440120.pdf","citationCount":"0","resultStr":"{\"title\":\"Budd-Chiari Syndrome as an Initial Presentation of Systemic Lupus Erythematosus Associated with Antiphospholipid Syndrome: A Case Report with Review of the Literature.\",\"authors\":\"Gashaw Solela, Merga Daba\",\"doi\":\"10.2147/OARRR.S425535\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Budd-Chiari syndrome (BCS) is a rare disorder characterized by hepatic outflow obstruction. It can be classified as primary or secondary BCS. Common causes of BCS include myeloproliferative diseases, infections, malignancies, and systemic autoimmune illnesses. Systemic lupus erythematosus (SLE) can be complicated with BCS. However, only a few case reports have described the uncommon occurrence of BCS as a primary presentation of SLE.</p><p><strong>Case presentation: </strong>We report the case of a 32-year-old female patient who presented with progressive abdominal distension of four months. On the abdominal CT scan, the left and middle hepatic veins were not visualized; the right hepatic vein and intrahepatic IVC had luminal narrowing; and there was caudate lobe enlargement suggestive of Budd-Chiari syndrome (BCS). Six months after the diagnosis of BCS, the patient developed other clinical features suggestive of systemic lupus erythematosus (SLE) and was finally diagnosed with SLE.</p><p><strong>Conclusion: </strong>Acquired or inherited thrombotic conditions are the most common underlying causes of Budd-Chiari syndrome. Systemic lupus erythematosus (SLE) is the most common cause of secondary APS and most patients present with Budd-Chiari syndrome as a manifestation of APS after the diagnosis of SLE. In rare cases, such as the current case, Budd-Chiari syndrome can present even before the diagnosis of SLE. Hence, we would like to emphasize that Budd-Chiari syndrome can be an initial presentation of SLE.</p>\",\"PeriodicalId\":45545,\"journal\":{\"name\":\"Open Access Rheumatology-Research and Reviews\",\"volume\":\"15 \",\"pages\":\"139-143\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/06/1b/oarrr-15-139.PMC10440120.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Open Access Rheumatology-Research and Reviews\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/OARRR.S425535\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"RHEUMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Access Rheumatology-Research and Reviews","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/OARRR.S425535","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
Budd-Chiari Syndrome as an Initial Presentation of Systemic Lupus Erythematosus Associated with Antiphospholipid Syndrome: A Case Report with Review of the Literature.
Introduction: Budd-Chiari syndrome (BCS) is a rare disorder characterized by hepatic outflow obstruction. It can be classified as primary or secondary BCS. Common causes of BCS include myeloproliferative diseases, infections, malignancies, and systemic autoimmune illnesses. Systemic lupus erythematosus (SLE) can be complicated with BCS. However, only a few case reports have described the uncommon occurrence of BCS as a primary presentation of SLE.
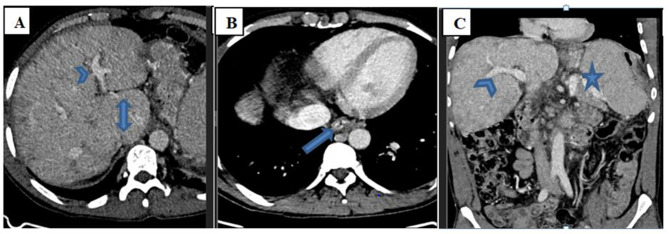
Case presentation: We report the case of a 32-year-old female patient who presented with progressive abdominal distension of four months. On the abdominal CT scan, the left and middle hepatic veins were not visualized; the right hepatic vein and intrahepatic IVC had luminal narrowing; and there was caudate lobe enlargement suggestive of Budd-Chiari syndrome (BCS). Six months after the diagnosis of BCS, the patient developed other clinical features suggestive of systemic lupus erythematosus (SLE) and was finally diagnosed with SLE.
Conclusion: Acquired or inherited thrombotic conditions are the most common underlying causes of Budd-Chiari syndrome. Systemic lupus erythematosus (SLE) is the most common cause of secondary APS and most patients present with Budd-Chiari syndrome as a manifestation of APS after the diagnosis of SLE. In rare cases, such as the current case, Budd-Chiari syndrome can present even before the diagnosis of SLE. Hence, we would like to emphasize that Budd-Chiari syndrome can be an initial presentation of SLE.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


