James J M Loan, Steven Tominey, Kirun Baweja, Julie Woodfield, Thomas J G Chambers, Mark Haley, Simran S Kundu, H Y Josephine Tang, Anthony N Wiggins, Michael T C Poon, Paul M Brennan
{"title":"英国和爱尔兰蛛网膜下腔出血后低钠血症筛查、调查和管理的前瞻性多中心研究","authors":"James J M Loan, Steven Tominey, Kirun Baweja, Julie Woodfield, Thomas J G Chambers, Mark Haley, Simran S Kundu, H Y Josephine Tang, Anthony N Wiggins, Michael T C Poon, Paul M Brennan","doi":"10.1136/svn-2022-001583","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Hyponatraemia often occurs after subarachnoid haemorrhage (SAH). However, its clinical significance and optimal management are uncertain. We audited the screening, investigation and management of hyponatraemia after SAH.</p><p><strong>Methods: </strong>We prospectively identified consecutive patients with spontaneous SAH admitted to neurosurgical units in the United Kingdom or Ireland. We reviewed medical records daily from admission to discharge, 21 days or death and extracted all measurements of serum sodium to identify hyponatraemia (<135 mmol/L). Main outcomes were death/dependency at discharge or 21 days and admission duration >10 days. Associations of hyponatraemia with outcome were assessed using logistic regression with adjustment for predictors of outcome after SAH and admission duration. We assessed hyponatraemia-free survival using multivariable Cox regression.</p><p><strong>Results: </strong>175/407 (43%) patients admitted to 24 neurosurgical units developed hyponatraemia. 5976 serum sodium measurements were made. Serum osmolality, urine osmolality and urine sodium were measured in 30/166 (18%) hyponatraemic patients with complete data. The most frequently target daily fluid intake was >3 L and this did not differ during hyponatraemic or non-hyponatraemic episodes. 26% (n/N=42/164) patients with hyponatraemia received sodium supplementation. 133 (35%) patients were dead or dependent within the study period and 240 (68%) patients had hospital admission for over 10 days. In the multivariable analyses, hyponatraemia was associated with less dependency (adjusted OR (aOR)=0.35 (95% CI 0.17 to 0.69)) but longer admissions (aOR=3.2 (1.8 to 5.7)). World Federation of Neurosurgical Societies grade I-III, modified Fisher 2-4 and posterior circulation aneurysms were associated with greater hazards of hyponatraemia.</p><p><strong>Conclusions: </strong>In this comprehensive multicentre prospective-adjusted analysis of patients with SAH, hyponatraemia was investigated inconsistently and, for most patients, was not associated with changes in management or clinical outcome. This work establishes a basis for the development of evidence-based SAH-specific guidance for targeted screening, investigation and management of high-risk patients to minimise the impact of hyponatraemia on admission duration and to improve consistency of patient care.</p>","PeriodicalId":22021,"journal":{"name":"Stroke and Vascular Neurology","volume":"8 3","pages":"207-216"},"PeriodicalIF":4.9000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10359796/pdf/","citationCount":"0","resultStr":"{\"title\":\"Prospective, multicentre study of screening, investigation and management of hyponatraemia after subarachnoid haemorrhage in the UK and Ireland.\",\"authors\":\"James J M Loan, Steven Tominey, Kirun Baweja, Julie Woodfield, Thomas J G Chambers, Mark Haley, Simran S Kundu, H Y Josephine Tang, Anthony N Wiggins, Michael T C Poon, Paul M Brennan\",\"doi\":\"10.1136/svn-2022-001583\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Hyponatraemia often occurs after subarachnoid haemorrhage (SAH). However, its clinical significance and optimal management are uncertain. We audited the screening, investigation and management of hyponatraemia after SAH.</p><p><strong>Methods: </strong>We prospectively identified consecutive patients with spontaneous SAH admitted to neurosurgical units in the United Kingdom or Ireland. We reviewed medical records daily from admission to discharge, 21 days or death and extracted all measurements of serum sodium to identify hyponatraemia (<135 mmol/L). Main outcomes were death/dependency at discharge or 21 days and admission duration >10 days. Associations of hyponatraemia with outcome were assessed using logistic regression with adjustment for predictors of outcome after SAH and admission duration. We assessed hyponatraemia-free survival using multivariable Cox regression.</p><p><strong>Results: </strong>175/407 (43%) patients admitted to 24 neurosurgical units developed hyponatraemia. 5976 serum sodium measurements were made. Serum osmolality, urine osmolality and urine sodium were measured in 30/166 (18%) hyponatraemic patients with complete data. The most frequently target daily fluid intake was >3 L and this did not differ during hyponatraemic or non-hyponatraemic episodes. 26% (n/N=42/164) patients with hyponatraemia received sodium supplementation. 133 (35%) patients were dead or dependent within the study period and 240 (68%) patients had hospital admission for over 10 days. In the multivariable analyses, hyponatraemia was associated with less dependency (adjusted OR (aOR)=0.35 (95% CI 0.17 to 0.69)) but longer admissions (aOR=3.2 (1.8 to 5.7)). World Federation of Neurosurgical Societies grade I-III, modified Fisher 2-4 and posterior circulation aneurysms were associated with greater hazards of hyponatraemia.</p><p><strong>Conclusions: </strong>In this comprehensive multicentre prospective-adjusted analysis of patients with SAH, hyponatraemia was investigated inconsistently and, for most patients, was not associated with changes in management or clinical outcome. This work establishes a basis for the development of evidence-based SAH-specific guidance for targeted screening, investigation and management of high-risk patients to minimise the impact of hyponatraemia on admission duration and to improve consistency of patient care.</p>\",\"PeriodicalId\":22021,\"journal\":{\"name\":\"Stroke and Vascular Neurology\",\"volume\":\"8 3\",\"pages\":\"207-216\"},\"PeriodicalIF\":4.9000,\"publicationDate\":\"2023-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10359796/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Stroke and Vascular Neurology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1136/svn-2022-001583\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Stroke and Vascular Neurology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/svn-2022-001583","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:低钠血症常发生在蛛网膜下腔出血(SAH)后。然而,其临床意义和最佳治疗尚不确定。我们审核了SAH后低钠血症的筛查、调查和处理。方法:我们前瞻性地确定了在英国或爱尔兰神经外科住院的连续自发性SAH患者。我们每天回顾从入院到出院、21天或死亡的医疗记录,并提取血清钠的所有测量值以确定低钠血症(10天)。使用逻辑回归评估低钠血症与预后的关系,并调整SAH后预后的预测因子和入院时间。我们使用多变量Cox回归评估无低钠血症生存率。结果:24个神经外科单元收治的患者中有175/407例(43%)发生低钠血症。测定5976例血清钠。测定了30/166例(18%)低钠血症患者的血清渗透压、尿渗透压和尿钠。最常见的目标每日液体摄入量是> 3l,这在低钠血症和非低钠血症发作期间没有差异。26% (n/ n =42/164)的低钠血症患者补充了钠。133例(35%)患者在研究期间死亡或依赖,240例(68%)患者住院时间超过10天。在多变量分析中,低钠血症与依赖性较低相关(调整后的OR (aOR)=0.35 (95% CI 0.17 - 0.69)),但入院时间较长(aOR=3.2(1.8 - 5.7))。世界神经外科学会联合会I-III级、改良Fisher 2-4级和后循环动脉瘤与低钠血症的危险性较大相关。结论:在这项针对SAH患者的综合多中心前瞻性调整分析中,对低钠血症的调查不一致,而且对大多数患者来说,低钠血症与治疗或临床结果的改变无关。这项工作为制定以证据为基础的针对高危患者的针对性筛查、调查和管理指南奠定了基础,以最大限度地减少低钠血症对入院时间的影响,并提高患者护理的一致性。
Prospective, multicentre study of screening, investigation and management of hyponatraemia after subarachnoid haemorrhage in the UK and Ireland.
Background: Hyponatraemia often occurs after subarachnoid haemorrhage (SAH). However, its clinical significance and optimal management are uncertain. We audited the screening, investigation and management of hyponatraemia after SAH.
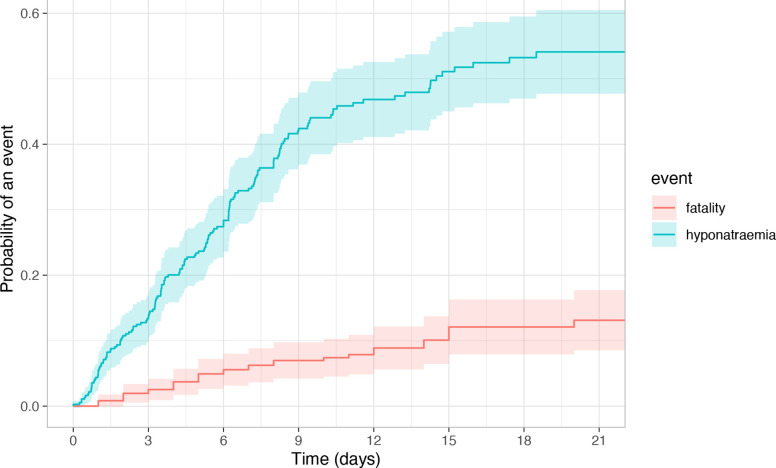
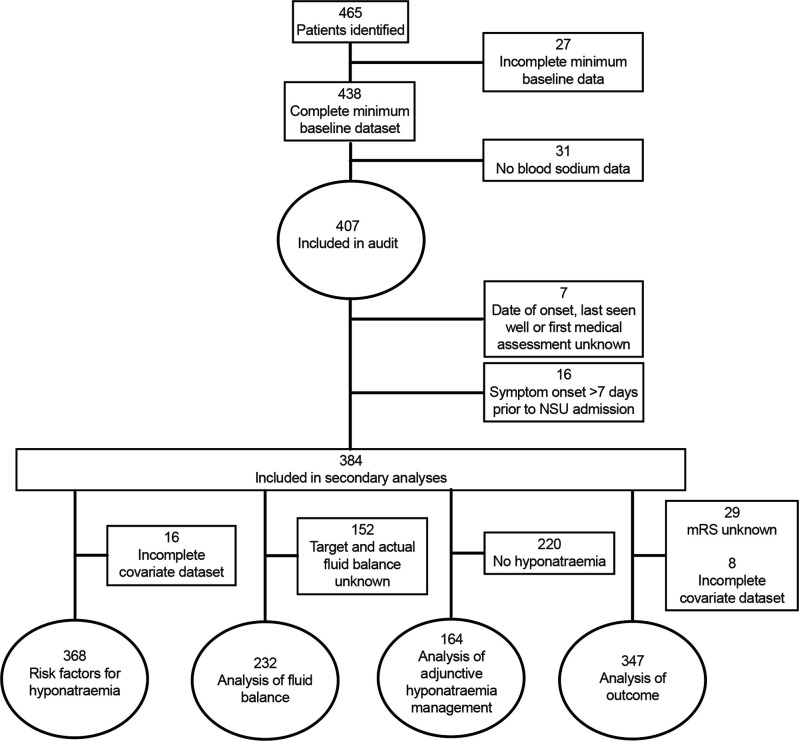
Methods: We prospectively identified consecutive patients with spontaneous SAH admitted to neurosurgical units in the United Kingdom or Ireland. We reviewed medical records daily from admission to discharge, 21 days or death and extracted all measurements of serum sodium to identify hyponatraemia (<135 mmol/L). Main outcomes were death/dependency at discharge or 21 days and admission duration >10 days. Associations of hyponatraemia with outcome were assessed using logistic regression with adjustment for predictors of outcome after SAH and admission duration. We assessed hyponatraemia-free survival using multivariable Cox regression.
Results: 175/407 (43%) patients admitted to 24 neurosurgical units developed hyponatraemia. 5976 serum sodium measurements were made. Serum osmolality, urine osmolality and urine sodium were measured in 30/166 (18%) hyponatraemic patients with complete data. The most frequently target daily fluid intake was >3 L and this did not differ during hyponatraemic or non-hyponatraemic episodes. 26% (n/N=42/164) patients with hyponatraemia received sodium supplementation. 133 (35%) patients were dead or dependent within the study period and 240 (68%) patients had hospital admission for over 10 days. In the multivariable analyses, hyponatraemia was associated with less dependency (adjusted OR (aOR)=0.35 (95% CI 0.17 to 0.69)) but longer admissions (aOR=3.2 (1.8 to 5.7)). World Federation of Neurosurgical Societies grade I-III, modified Fisher 2-4 and posterior circulation aneurysms were associated with greater hazards of hyponatraemia.
Conclusions: In this comprehensive multicentre prospective-adjusted analysis of patients with SAH, hyponatraemia was investigated inconsistently and, for most patients, was not associated with changes in management or clinical outcome. This work establishes a basis for the development of evidence-based SAH-specific guidance for targeted screening, investigation and management of high-risk patients to minimise the impact of hyponatraemia on admission duration and to improve consistency of patient care.
期刊介绍:
Stroke and Vascular Neurology (SVN) is the official journal of the Chinese Stroke Association. Supported by a team of renowned Editors, and fully Open Access, the journal encourages debate on controversial techniques, issues on health policy and social medicine.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


