Ahmad Mahdi Ahmad, Aya Ibrahim Elshenawy, Mohammed Abdelghany, Heba Ali Abd Elghaffar
{"title":"早期康复计划对急性心力衰竭住院患者的功能能力、日常生活活动和 N 端前体脑钠肽的影响。随机对照试验。","authors":"Ahmad Mahdi Ahmad, Aya Ibrahim Elshenawy, Mohammed Abdelghany, Heba Ali Abd Elghaffar","doi":"10.1142/S1013702523500014","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients hospitalised for acute decompensated heart failure (ADHF) show reduced functional capacity, limited activities of daily living (ADL), and elevated N-terminal prohormone of brain natriuretic peptide (NT-proBNP). The management of these patients focuses mainly on medical therapy with little consideration for in-patient cardiac rehabilitation. There has been a growing interest in evaluating the efficacy of early mobilisation, as the core for in-hospital rehabilitation, in ADHF patients in the last decade; however, the randomised trials on this topic are few.</p><p><strong>Objective: </strong>This randomised-controlled study, therefore, aimed to further test the hypothesis that early supervised mobilisation would have beneficial effects on functional capacity, ADL, and NT-proBNP in stabilised patients following ADHF.</p><p><strong>Methods: </strong>This is a single-centered, randomised-controlled, parallel-group trial in which 30 patients hospitalised for ADHF were randomly assigned to two groups; the study group (<math><mstyle><mtext>age</mtext></mstyle><mo>=</mo><mn>55</mn><mo>.</mo><mn>4</mn><mo>±</mo><mn>5</mn><mo>.</mo><mn>46</mn></math> years, <math><msub><mrow><mi>n</mi></mrow><mrow><mn>1</mn></mrow></msub><mo>=</mo><mn>15</mn></math>) and the control group (<math><mstyle><mtext>age</mtext></mstyle><mo>=</mo><mn>55</mn><mo>.</mo><mn>73</mn><mo>±</mo><mn>5</mn><mo>.</mo><mn>61</mn></math> years, <math><msub><mrow><mi>n</mi></mrow><mrow><mn>2</mn></mrow></msub></math>=15). Inclusion criteria were ADHF on top of chronic heart failure independent of etiology or ejection fraction, clinical/hemodynamic stability, age from 40 to 60 years old, and both genders. Exclusion criteria were cardiogenic shock, acute coronary ischemia, or significant arrhythmia. Both groups received the usual medical care, but only the study group received an early structured mobilisation protocol within 3 days of hospital admission till discharge. The outcome measures were the 6-min walk distance (6-MWD) and the rating of perceived exertion (RPE) determined from the 6-min walk test at discharge, the Barthel index (BI), NT-proBNP, and the length of hospital stays (LOS).</p><p><strong>Results: </strong>The study group showed significantly greater improvements compared to the controls in the 6-MWD (<math><mn>252</mn><mo>.</mo><mn>28</mn><mo>±</mo><mn>92</mn><mo>.</mo><mn>32</mn></math> versus <math><mn>106</mn><mo>.</mo><mn>35</mn><mo>±</mo><mn>56</mn><mo>.</mo><mn>36</mn></math> m, <math><mi>P</mi><mo><</mo><mn>0</mn><mo>.</mo><mn>001</mn></math>), the RPE (<math><mn>12</mn><mo>.</mo><mn>53</mn><mo>±</mo><mn>0</mn><mo>.</mo><mn>91</mn></math> versus <math><mn>15</mn><mo>.</mo><mn>4</mn><mo>±</mo><mn>1</mn><mo>.</mo><mn>63</mn></math>, <math><mi>P</mi><mo><</mo><mn>0</mn><mo>.</mo><mn>001</mn></math>), and the LOS (<math><mn>10</mn><mo>.</mo><mn>42</mn><mo>±</mo><mn>4</mn><mo>.</mo><mn>23</mn></math> versus <math><mn>16</mn><mo>.</mo><mn>85</mn><mo>±</mo><mn>6</mn><mo>.</mo><mn>87</mn></math> days, <math><mi>p</mi><mo>=</mo><mn>0</mn><mo>.</mo><mn>009</mn></math>) at discharge. Also, the study group showed significant improvements in the BI compared to baseline [100 (100-100) versus 41.87 (35-55), <math><mi>p</mi><mo>=</mo><mn>0</mn><mo>.</mo><mn>009</mn></math>] and the controls [100 (100-100) versus 92.5(85-95), <math><mi>p</mi><mo>=</mo><mn>0</mn><mo>.</mo><mn>006</mn></math>]. The mean value of NT-proBNP showed a significant reduction only compared to baseline (<math><mn>786</mn><mo>.</mo><mn>28</mn><mo>±</mo><mn>269</mn><mo>.</mo><mn>5</mn></math> versus <math><mn>1069</mn><mo>.</mo><mn>03</mn><mo>±</mo><mn>528</mn><mo>.</mo><mn>87</mn></math> pg/mL, <math><mi>p</mi><mo>=</mo><mn>0</mn><mo>.</mo><mn>04</mn></math>) following the intervention. The absolute mean change (<math><mi>Δ</mi></math>) of NT-proBNP showed an observed difference between groups in favor of the study group (i.e., <math><mi>Δ</mi><mo>=</mo><mi>↓</mi><mn>282</mn><mo>.</mo><mn>75</mn><mo>±</mo><mn>494</mn><mo>.</mo><mn>13</mn></math> pg/mL in the study group versus <math><mi>↓</mi><mn>26</mn><mo>.</mo><mn>42</mn><mo>±</mo><mn>222</mn><mo>.</mo><mn>21</mn></math> pg/mL in the control group, <math><mi>p</mi><mo>=</mo><mn>0</mn><mo>.</mo><mn>077</mn></math>).</p><p><strong>Conclusion: </strong>Early structured mobilisation under the supervision of a physiotherapist could be strongly suggested in combination with the usual medical care to help improve the functional capacity and daily living activities, reduce NT-proBNP levels, and shorten the hospital stay in stabilised patients following ADHF. Trial registration number: PACTR202202476383975.</p>","PeriodicalId":0,"journal":{"name":"","volume":null,"pages":null},"PeriodicalIF":0.0,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e5/e1/hkpj-43-019.PMC10423683.pdf","citationCount":"0","resultStr":"{\"title\":\"Effects of early mobilisation program on functional capacity, daily living activities, and N-terminal prohormone brain natriuretic peptide in patients hospitalised for acute heart failure. A randomised controlled trial.\",\"authors\":\"Ahmad Mahdi Ahmad, Aya Ibrahim Elshenawy, Mohammed Abdelghany, Heba Ali Abd Elghaffar\",\"doi\":\"10.1142/S1013702523500014\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Patients hospitalised for acute decompensated heart failure (ADHF) show reduced functional capacity, limited activities of daily living (ADL), and elevated N-terminal prohormone of brain natriuretic peptide (NT-proBNP). The management of these patients focuses mainly on medical therapy with little consideration for in-patient cardiac rehabilitation. There has been a growing interest in evaluating the efficacy of early mobilisation, as the core for in-hospital rehabilitation, in ADHF patients in the last decade; however, the randomised trials on this topic are few.</p><p><strong>Objective: </strong>This randomised-controlled study, therefore, aimed to further test the hypothesis that early supervised mobilisation would have beneficial effects on functional capacity, ADL, and NT-proBNP in stabilised patients following ADHF.</p><p><strong>Methods: </strong>This is a single-centered, randomised-controlled, parallel-group trial in which 30 patients hospitalised for ADHF were randomly assigned to two groups; the study group (<math><mstyle><mtext>age</mtext></mstyle><mo>=</mo><mn>55</mn><mo>.</mo><mn>4</mn><mo>±</mo><mn>5</mn><mo>.</mo><mn>46</mn></math> years, <math><msub><mrow><mi>n</mi></mrow><mrow><mn>1</mn></mrow></msub><mo>=</mo><mn>15</mn></math>) and the control group (<math><mstyle><mtext>age</mtext></mstyle><mo>=</mo><mn>55</mn><mo>.</mo><mn>73</mn><mo>±</mo><mn>5</mn><mo>.</mo><mn>61</mn></math> years, <math><msub><mrow><mi>n</mi></mrow><mrow><mn>2</mn></mrow></msub></math>=15). Inclusion criteria were ADHF on top of chronic heart failure independent of etiology or ejection fraction, clinical/hemodynamic stability, age from 40 to 60 years old, and both genders. Exclusion criteria were cardiogenic shock, acute coronary ischemia, or significant arrhythmia. Both groups received the usual medical care, but only the study group received an early structured mobilisation protocol within 3 days of hospital admission till discharge. The outcome measures were the 6-min walk distance (6-MWD) and the rating of perceived exertion (RPE) determined from the 6-min walk test at discharge, the Barthel index (BI), NT-proBNP, and the length of hospital stays (LOS).</p><p><strong>Results: </strong>The study group showed significantly greater improvements compared to the controls in the 6-MWD (<math><mn>252</mn><mo>.</mo><mn>28</mn><mo>±</mo><mn>92</mn><mo>.</mo><mn>32</mn></math> versus <math><mn>106</mn><mo>.</mo><mn>35</mn><mo>±</mo><mn>56</mn><mo>.</mo><mn>36</mn></math> m, <math><mi>P</mi><mo><</mo><mn>0</mn><mo>.</mo><mn>001</mn></math>), the RPE (<math><mn>12</mn><mo>.</mo><mn>53</mn><mo>±</mo><mn>0</mn><mo>.</mo><mn>91</mn></math> versus <math><mn>15</mn><mo>.</mo><mn>4</mn><mo>±</mo><mn>1</mn><mo>.</mo><mn>63</mn></math>, <math><mi>P</mi><mo><</mo><mn>0</mn><mo>.</mo><mn>001</mn></math>), and the LOS (<math><mn>10</mn><mo>.</mo><mn>42</mn><mo>±</mo><mn>4</mn><mo>.</mo><mn>23</mn></math> versus <math><mn>16</mn><mo>.</mo><mn>85</mn><mo>±</mo><mn>6</mn><mo>.</mo><mn>87</mn></math> days, <math><mi>p</mi><mo>=</mo><mn>0</mn><mo>.</mo><mn>009</mn></math>) at discharge. Also, the study group showed significant improvements in the BI compared to baseline [100 (100-100) versus 41.87 (35-55), <math><mi>p</mi><mo>=</mo><mn>0</mn><mo>.</mo><mn>009</mn></math>] and the controls [100 (100-100) versus 92.5(85-95), <math><mi>p</mi><mo>=</mo><mn>0</mn><mo>.</mo><mn>006</mn></math>]. The mean value of NT-proBNP showed a significant reduction only compared to baseline (<math><mn>786</mn><mo>.</mo><mn>28</mn><mo>±</mo><mn>269</mn><mo>.</mo><mn>5</mn></math> versus <math><mn>1069</mn><mo>.</mo><mn>03</mn><mo>±</mo><mn>528</mn><mo>.</mo><mn>87</mn></math> pg/mL, <math><mi>p</mi><mo>=</mo><mn>0</mn><mo>.</mo><mn>04</mn></math>) following the intervention. The absolute mean change (<math><mi>Δ</mi></math>) of NT-proBNP showed an observed difference between groups in favor of the study group (i.e., <math><mi>Δ</mi><mo>=</mo><mi>↓</mi><mn>282</mn><mo>.</mo><mn>75</mn><mo>±</mo><mn>494</mn><mo>.</mo><mn>13</mn></math> pg/mL in the study group versus <math><mi>↓</mi><mn>26</mn><mo>.</mo><mn>42</mn><mo>±</mo><mn>222</mn><mo>.</mo><mn>21</mn></math> pg/mL in the control group, <math><mi>p</mi><mo>=</mo><mn>0</mn><mo>.</mo><mn>077</mn></math>).</p><p><strong>Conclusion: </strong>Early structured mobilisation under the supervision of a physiotherapist could be strongly suggested in combination with the usual medical care to help improve the functional capacity and daily living activities, reduce NT-proBNP levels, and shorten the hospital stay in stabilised patients following ADHF. Trial registration number: PACTR202202476383975.</p>\",\"PeriodicalId\":0,\"journal\":{\"name\":\"\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":0.0,\"publicationDate\":\"2023-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e5/e1/hkpj-43-019.PMC10423683.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1142/S1013702523500014\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/10/10 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1142/S1013702523500014","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/10/10 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Effects of early mobilisation program on functional capacity, daily living activities, and N-terminal prohormone brain natriuretic peptide in patients hospitalised for acute heart failure. A randomised controlled trial.
Background: Patients hospitalised for acute decompensated heart failure (ADHF) show reduced functional capacity, limited activities of daily living (ADL), and elevated N-terminal prohormone of brain natriuretic peptide (NT-proBNP). The management of these patients focuses mainly on medical therapy with little consideration for in-patient cardiac rehabilitation. There has been a growing interest in evaluating the efficacy of early mobilisation, as the core for in-hospital rehabilitation, in ADHF patients in the last decade; however, the randomised trials on this topic are few.
Objective: This randomised-controlled study, therefore, aimed to further test the hypothesis that early supervised mobilisation would have beneficial effects on functional capacity, ADL, and NT-proBNP in stabilised patients following ADHF.
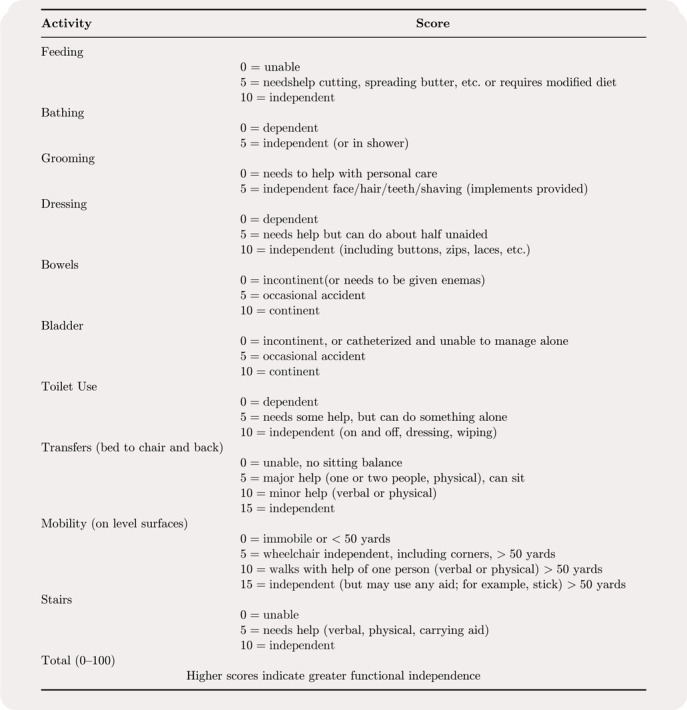
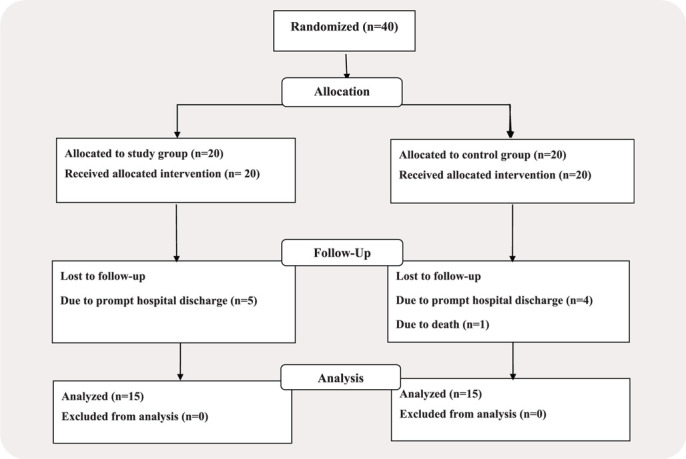
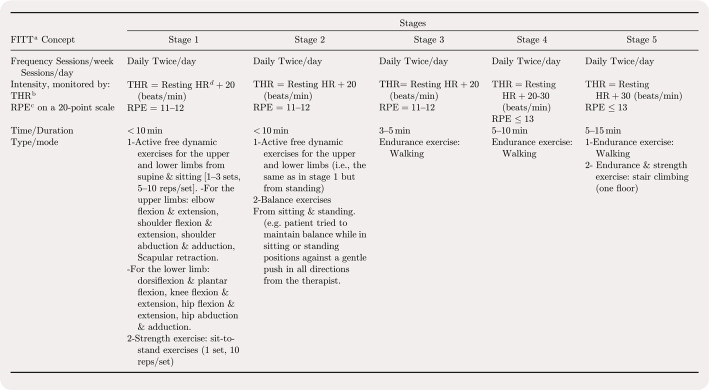
Methods: This is a single-centered, randomised-controlled, parallel-group trial in which 30 patients hospitalised for ADHF were randomly assigned to two groups; the study group ( years, ) and the control group ( years, =15). Inclusion criteria were ADHF on top of chronic heart failure independent of etiology or ejection fraction, clinical/hemodynamic stability, age from 40 to 60 years old, and both genders. Exclusion criteria were cardiogenic shock, acute coronary ischemia, or significant arrhythmia. Both groups received the usual medical care, but only the study group received an early structured mobilisation protocol within 3 days of hospital admission till discharge. The outcome measures were the 6-min walk distance (6-MWD) and the rating of perceived exertion (RPE) determined from the 6-min walk test at discharge, the Barthel index (BI), NT-proBNP, and the length of hospital stays (LOS).
Results: The study group showed significantly greater improvements compared to the controls in the 6-MWD ( versus m, ), the RPE ( versus , ), and the LOS ( versus days, ) at discharge. Also, the study group showed significant improvements in the BI compared to baseline [100 (100-100) versus 41.87 (35-55), ] and the controls [100 (100-100) versus 92.5(85-95), ]. The mean value of NT-proBNP showed a significant reduction only compared to baseline ( versus pg/mL, ) following the intervention. The absolute mean change () of NT-proBNP showed an observed difference between groups in favor of the study group (i.e., pg/mL in the study group versus pg/mL in the control group, ).
Conclusion: Early structured mobilisation under the supervision of a physiotherapist could be strongly suggested in combination with the usual medical care to help improve the functional capacity and daily living activities, reduce NT-proBNP levels, and shorten the hospital stay in stabilised patients following ADHF. Trial registration number: PACTR202202476383975.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


