Natassia Tan, John Lubel, William Kemp, Stuart Roberts, Ammar Majeed
{"title":"Current Therapeutics in Primary Sclerosing Cholangitis.","authors":"Natassia Tan, John Lubel, William Kemp, Stuart Roberts, Ammar Majeed","doi":"10.14218/JCTH.2022.00068S","DOIUrl":null,"url":null,"abstract":"<p><p>Primary sclerosing cholangitis (PSC) is an orphan, cholestatic liver disease that is characterized by inflammatory biliary strictures with variable progression to end-stage liver disease. Its pathophysiology is poorly understood. Chronic biliary inflammation is likely driven by immune dysregulation, gut dysbiosis, and environmental exposures resulting in gut-liver crosstalk and bile acid metabolism disturbances. There is no proven medical therapy that alters disease progression in PSC, with the commonly prescribed ursodeoxycholic acid being shown to improve liver biochemistry at low-moderate doses (15-23 mg/kg/day) but not alter transplant-free survival or liver-related outcomes. Liver transplantation is the only option for patients who develop end-stage liver disease or refractory complications of PSC. Immunosuppressive and antifibrotic agents have not proven to be effective, but there is promise for manipulation of the gut microbiome with fecal microbiota transplantation and antibiotics. Bile acid manipulation via alternate synthetic bile acids such as norursodeoxycholic acid, or interaction at a transcriptional level via nuclear receptor agonists and fibrates have shown potential in phase II trials in PSC with several leading to larger phase III trials. In view of the enhanced malignancy risk, statins, and aspirin show potential for reducing the risk of colorectal cancer and cholangiocarcinoma in PSC patients. For patients who develop clinically relevant strictures with cholestatic symptoms and worsening liver function, balloon dilatation is safer compared with biliary stent insertion with equivalent clinical efficacy.</p>","PeriodicalId":15484,"journal":{"name":"Journal of Clinical and Translational Hepatology","volume":"11 5","pages":"1267-1281"},"PeriodicalIF":3.1000,"publicationDate":"2023-10-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/95/ee/JCTH-11-1267.PMC10412694.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical and Translational Hepatology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.14218/JCTH.2022.00068S","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/4/17 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
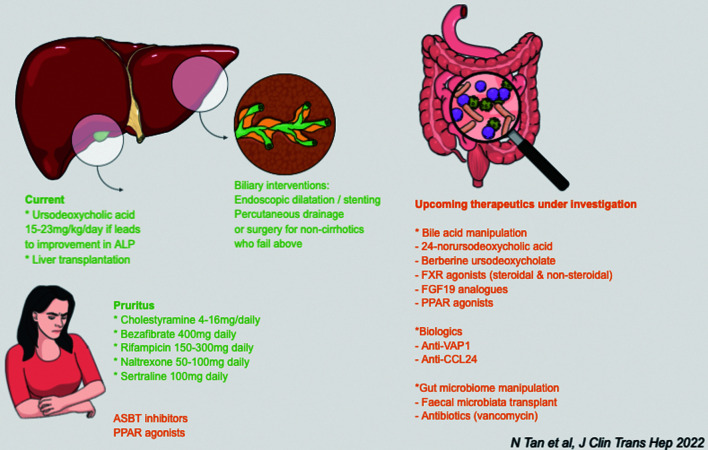
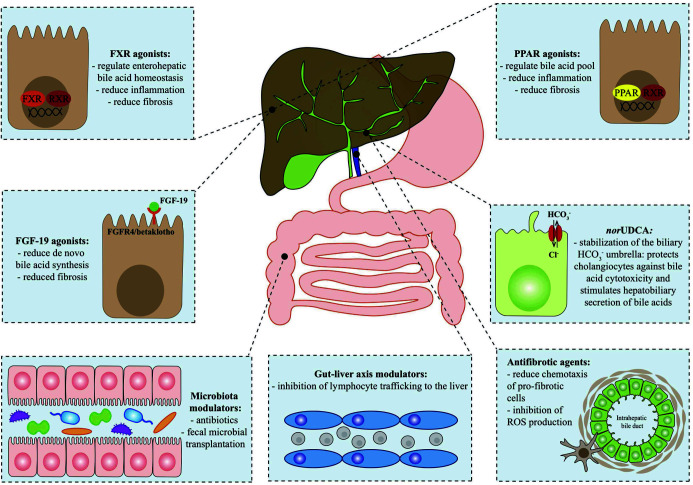
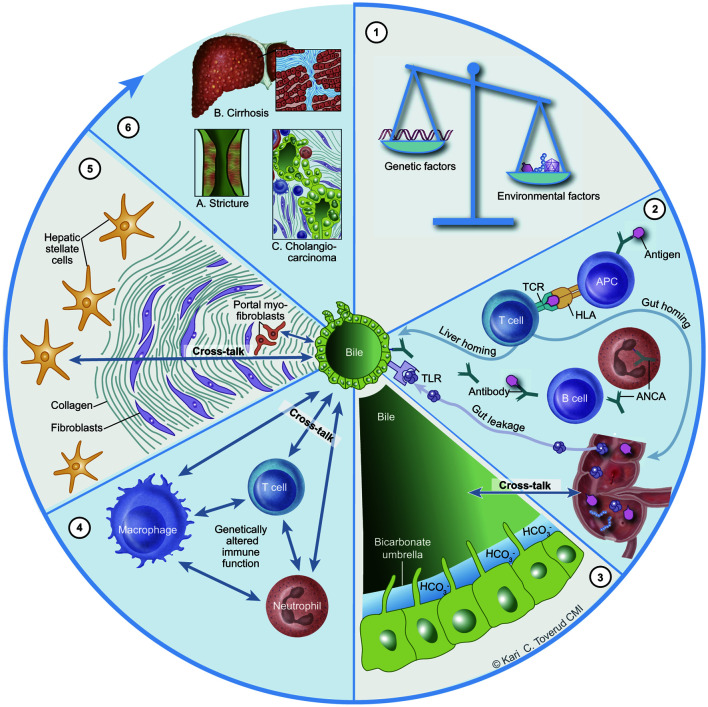
Primary sclerosing cholangitis (PSC) is an orphan, cholestatic liver disease that is characterized by inflammatory biliary strictures with variable progression to end-stage liver disease. Its pathophysiology is poorly understood. Chronic biliary inflammation is likely driven by immune dysregulation, gut dysbiosis, and environmental exposures resulting in gut-liver crosstalk and bile acid metabolism disturbances. There is no proven medical therapy that alters disease progression in PSC, with the commonly prescribed ursodeoxycholic acid being shown to improve liver biochemistry at low-moderate doses (15-23 mg/kg/day) but not alter transplant-free survival or liver-related outcomes. Liver transplantation is the only option for patients who develop end-stage liver disease or refractory complications of PSC. Immunosuppressive and antifibrotic agents have not proven to be effective, but there is promise for manipulation of the gut microbiome with fecal microbiota transplantation and antibiotics. Bile acid manipulation via alternate synthetic bile acids such as norursodeoxycholic acid, or interaction at a transcriptional level via nuclear receptor agonists and fibrates have shown potential in phase II trials in PSC with several leading to larger phase III trials. In view of the enhanced malignancy risk, statins, and aspirin show potential for reducing the risk of colorectal cancer and cholangiocarcinoma in PSC patients. For patients who develop clinically relevant strictures with cholestatic symptoms and worsening liver function, balloon dilatation is safer compared with biliary stent insertion with equivalent clinical efficacy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


