Keith Owen Yeates, Karen M Barlow, Bruce Wright, Ken Tang, Olesya Barrett, Edward Berdusco, Amanda M Black, Brenda Clark, Alf Conradi, Heather Godfrey, Ashley T Kolstad, Anh Ly, Angelo Mikrogianakis, Ross Purser, Kathryn Schneider, Antonia S Stang, Roger Zemek, Jennifer D Zwicker, David W Johnson
{"title":"Health care impact of implementing a clinical pathway for acute care of pediatric concussion: a stepped wedge, cluster randomised trial.","authors":"Keith Owen Yeates, Karen M Barlow, Bruce Wright, Ken Tang, Olesya Barrett, Edward Berdusco, Amanda M Black, Brenda Clark, Alf Conradi, Heather Godfrey, Ashley T Kolstad, Anh Ly, Angelo Mikrogianakis, Ross Purser, Kathryn Schneider, Antonia S Stang, Roger Zemek, Jennifer D Zwicker, David W Johnson","doi":"10.1007/s43678-023-00530-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To test the effects of actively implementing a clinical pathway for acute care of pediatric concussion on health care utilization and costs.</p><p><strong>Methods: </strong>Stepped wedge, cluster randomized trial of a clinical pathway, conducted in 5 emergency departments (ED) in Alberta, Canada from February 1 to November 30, 2019. The clinical pathway emphasized standardized assessment of risk for persistent symptoms, provision of consistent information to patients and families, and referral for outpatient follow-up. De-identified administrative data measured 6 outcomes: ED return visits; outpatient follow-up visits; length of ED stay, including total time, time from triage to physician initial assessment, and time from physician initial assessment to disposition; and total physician claims in an episode of care.</p><p><strong>Results: </strong>A total of 2878 unique patients (1164 female, 1713 male) aged 5-17 years (median 11.00, IQR 8, 14) met case criteria. They completed 3009 visits to the 5 sites and 781 follow-up visits to outpatient care, constituting 2910 episodes of care. Implementation did not alter the likelihood of an ED return visit (OR 0.77, 95% CI 0.39, 1.52), but increased the likelihood of outpatient follow-up visits (OR 1.84, 95% CI 1.19, 2.85). Total length of ED stay was unchanged, but time from physician initial assessment to disposition decreased significantly (mean change - 23.76 min, 95% CI - 37.99, - 9.52). Total physician claims increased significantly at only 1 of 5 sites.</p><p><strong>Conclusions: </strong>Implementation of a clinical pathway in the ED increased outpatient follow-up and reduced the time from physician initial assessment to disposition, without increasing physician costs. Implementation of a clinical pathway can align acute care of pediatric concussion more closely with existing clinical practice guidelines while making care more efficient.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov NCT05095012.</p>","PeriodicalId":55286,"journal":{"name":"Canadian Journal of Emergency Medicine","volume":"25 7","pages":"627-636"},"PeriodicalIF":2.0000,"publicationDate":"2023-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10333406/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s43678-023-00530-1","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: To test the effects of actively implementing a clinical pathway for acute care of pediatric concussion on health care utilization and costs.
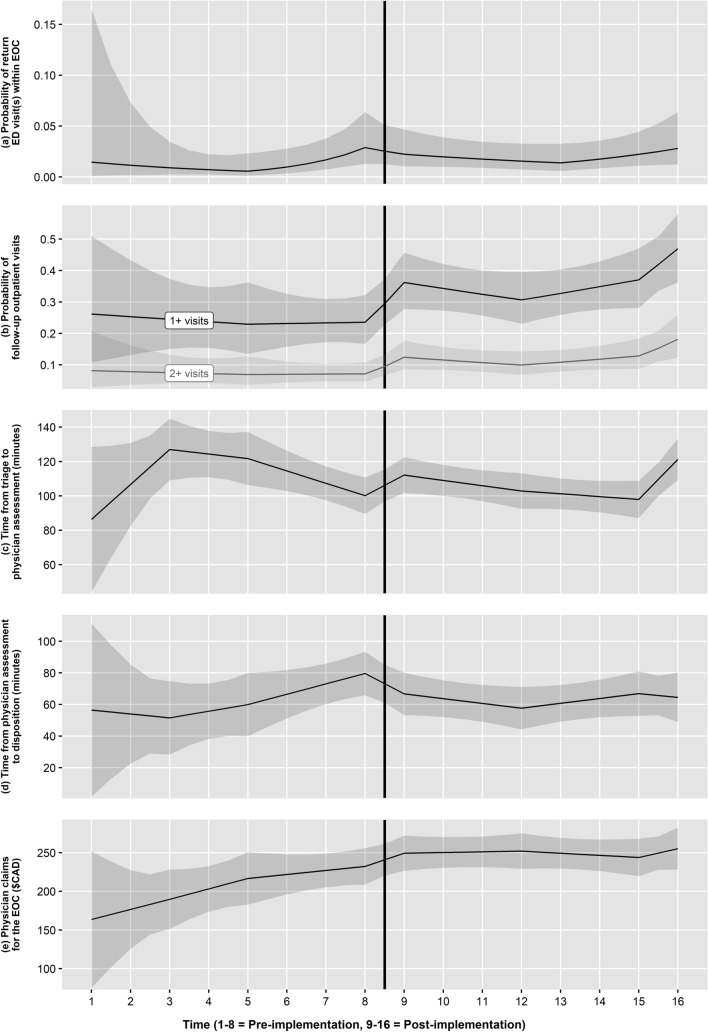
Methods: Stepped wedge, cluster randomized trial of a clinical pathway, conducted in 5 emergency departments (ED) in Alberta, Canada from February 1 to November 30, 2019. The clinical pathway emphasized standardized assessment of risk for persistent symptoms, provision of consistent information to patients and families, and referral for outpatient follow-up. De-identified administrative data measured 6 outcomes: ED return visits; outpatient follow-up visits; length of ED stay, including total time, time from triage to physician initial assessment, and time from physician initial assessment to disposition; and total physician claims in an episode of care.
Results: A total of 2878 unique patients (1164 female, 1713 male) aged 5-17 years (median 11.00, IQR 8, 14) met case criteria. They completed 3009 visits to the 5 sites and 781 follow-up visits to outpatient care, constituting 2910 episodes of care. Implementation did not alter the likelihood of an ED return visit (OR 0.77, 95% CI 0.39, 1.52), but increased the likelihood of outpatient follow-up visits (OR 1.84, 95% CI 1.19, 2.85). Total length of ED stay was unchanged, but time from physician initial assessment to disposition decreased significantly (mean change - 23.76 min, 95% CI - 37.99, - 9.52). Total physician claims increased significantly at only 1 of 5 sites.
Conclusions: Implementation of a clinical pathway in the ED increased outpatient follow-up and reduced the time from physician initial assessment to disposition, without increasing physician costs. Implementation of a clinical pathway can align acute care of pediatric concussion more closely with existing clinical practice guidelines while making care more efficient.
期刊介绍:
CJEM is a peer-reviewed journal owned by CAEP. CJEM is published every 2 months (January, March, May, July, September and November). CJEM presents articles of interest to emergency care providers in rural, urban or academic settings. Publishing services are provided by the Canadian Medical Association.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


