Deep brain stimulation in a pediatric dystonia patient with cochlear implants and mitochondrial disorder: novel application of a frameless stereotactic system and navigating the anesthesia choice and neurosurgical complexities. Illustrative case.
Audrey Grossen, Helen H Shi, Mallory Schenk, Amber Stocco, Justin Ramsey, Suneet Sahgal, Andrew K Conner, Virendra R Desai
{"title":"Deep brain stimulation in a pediatric dystonia patient with cochlear implants and mitochondrial disorder: novel application of a frameless stereotactic system and navigating the anesthesia choice and neurosurgical complexities. Illustrative case.","authors":"Audrey Grossen, Helen H Shi, Mallory Schenk, Amber Stocco, Justin Ramsey, Suneet Sahgal, Andrew K Conner, Virendra R Desai","doi":"10.3171/CASE23128","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>This report presents a case of medically refractory dystonia in a pediatric patient successfully treated with bilateral subthalamic nucleus (STN) deep brain stimulation (DBS) while under general anesthesia by using microelectrode recordings (MERs) with intraoperative computed tomography (CT).</p><p><strong>Observations: </strong>The patient was an 18-year-old female with primary dystonia secondary to mitochondrial Leigh syndrome. Her past medical history was significant for complex partial epilepsy and hearing loss treated with cochlear implants. Her cochlear implants precluded anatomical targeting via magnetic resonance imaging. Additionally, the patient could not tolerate awake surgery with MER. The decision was made to proceed with bilateral STN DBS with intraoperative CT with the patient under general anesthesia. The patient's cochlear implants made standard frame placement difficult, so navigation was performed with the Nexframe system. Recordings were obtained with the patient under general anesthesia with ketamine, dexmedetomidine, and remifentanil. At the 3- and 6-month follow-ups, the patient demonstrated marked improvement in dystonia without neurological complications.</p><p><strong>Lessons: </strong>This is the first case of dystonia secondary to Leigh syndrome treated with DBS. Additionally, the authors describe the novel use of the Nexframe for DBS lead placement in a pediatric patient. This demonstrates that STN DBS with the use of MER and intraoperative CT can be a safe and effective method of treating dystonia in certain pediatric patients.</p>","PeriodicalId":16554,"journal":{"name":"Journal of Neurosurgery: Case Lessons","volume":"6 6","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2023-08-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/98/6e/CASE23128.PMC10555587.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Neurosurgery: Case Lessons","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3171/CASE23128","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
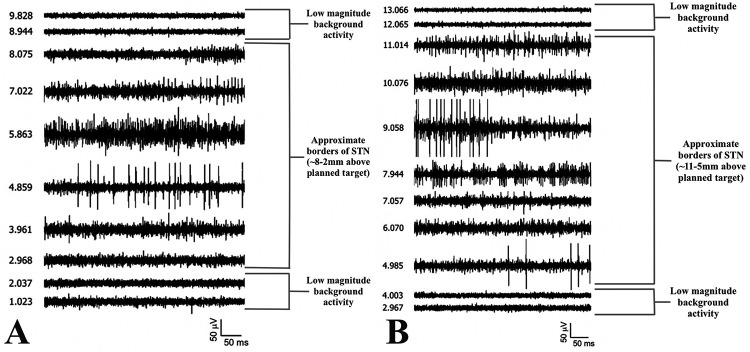
Background: This report presents a case of medically refractory dystonia in a pediatric patient successfully treated with bilateral subthalamic nucleus (STN) deep brain stimulation (DBS) while under general anesthesia by using microelectrode recordings (MERs) with intraoperative computed tomography (CT).
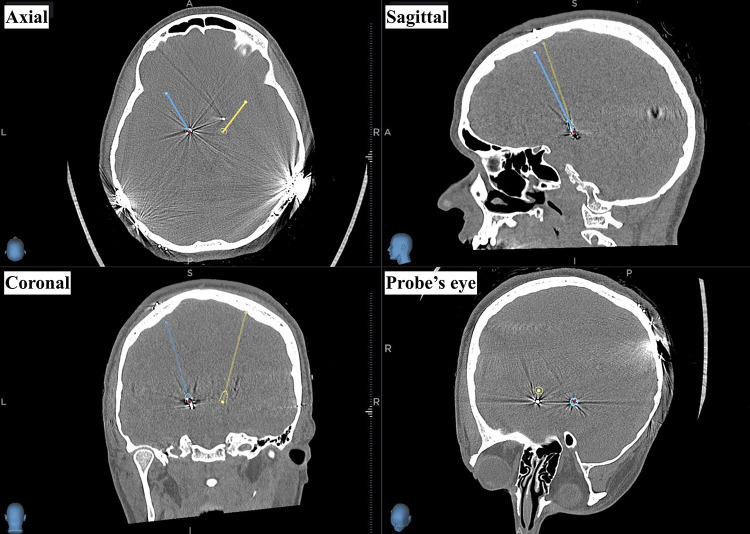
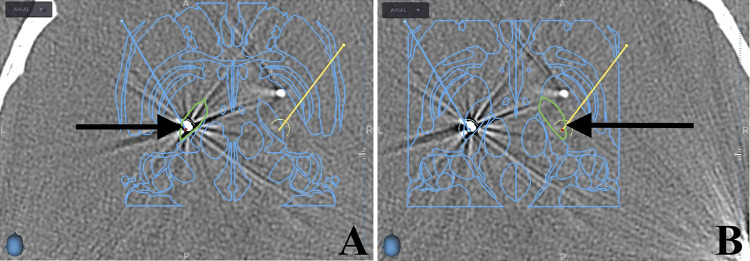
Observations: The patient was an 18-year-old female with primary dystonia secondary to mitochondrial Leigh syndrome. Her past medical history was significant for complex partial epilepsy and hearing loss treated with cochlear implants. Her cochlear implants precluded anatomical targeting via magnetic resonance imaging. Additionally, the patient could not tolerate awake surgery with MER. The decision was made to proceed with bilateral STN DBS with intraoperative CT with the patient under general anesthesia. The patient's cochlear implants made standard frame placement difficult, so navigation was performed with the Nexframe system. Recordings were obtained with the patient under general anesthesia with ketamine, dexmedetomidine, and remifentanil. At the 3- and 6-month follow-ups, the patient demonstrated marked improvement in dystonia without neurological complications.
Lessons: This is the first case of dystonia secondary to Leigh syndrome treated with DBS. Additionally, the authors describe the novel use of the Nexframe for DBS lead placement in a pediatric patient. This demonstrates that STN DBS with the use of MER and intraoperative CT can be a safe and effective method of treating dystonia in certain pediatric patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


