Preservation of Enlarged Mastoid Emissary Vein during Microvascular Decompression for Trigeminal Neuralgia Accompanied by Abnormal Venous Drainage: A Technical Case Report.
{"title":"Preservation of Enlarged Mastoid Emissary Vein during Microvascular Decompression for Trigeminal Neuralgia Accompanied by Abnormal Venous Drainage: A Technical Case Report.","authors":"Taku Sugiyama, Miki Fujimura","doi":"10.2176/jns-nmc.2023-0016","DOIUrl":null,"url":null,"abstract":"<p><p>During microvascular decompression (MVD) for trigeminal neuralgia (TGN), the mastoid emissary veins (MEV) are routinely sacrificed using the suboccipital retrosigmoid approach. The technical nuances when the MEV is an important collateral venous pathway for the obstructive internal jugular vein (IJV) have not been described thus far. Herein, we demonstrate for the first time a modified surgical technique for MVD to preserve the MEV. A 62-year-old man with a 10-year history of TGN refractory to carbamazepine was referred to our hospital for MVD. Preoperative imaging revealed that the superior cerebellar artery was the offending vessel. Computed tomography angiography also revealed that his contralateral IJV pathway was hypoplastic, and the ipsilateral pathway was severely stenosed by the external compression of the elongated styloid process and the transverse process of the first cervical vertebra. The ipsilateral MEV and the connecting occipital veins were enlarged as the sole collateral pathways of intracranial venous drainage. A modified MVD technique, including an upside-down L-shaped skin incision, layer-by-layer dissection of the occipital muscles, and denuding of the intraosseous part of the MEV, was used to cure the TGN with the preservation of the venous pathway. After surgery, the pain completely diminished without any complications. In conclusion, such technical modifications would be applicable in cases where the MEV needs to be preserved during posterior fossa surgery. Preoperative screening of the venous system is also recommended.</p>","PeriodicalId":19260,"journal":{"name":"NMC Case Report Journal","volume":"10 ","pages":"139-143"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/41/ba/2188-4226-10-0139.PMC10247221.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"NMC Case Report Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2176/jns-nmc.2023-0016","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
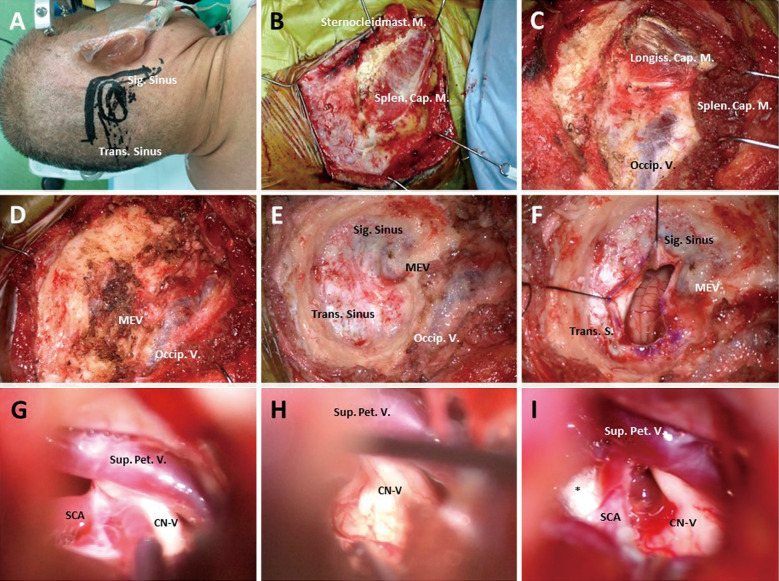
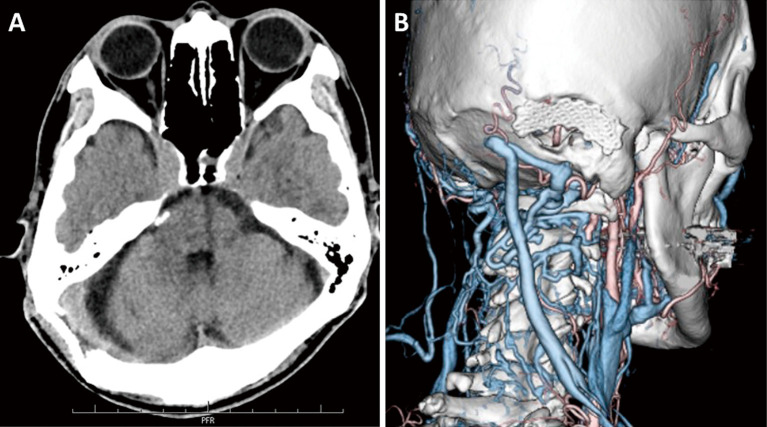
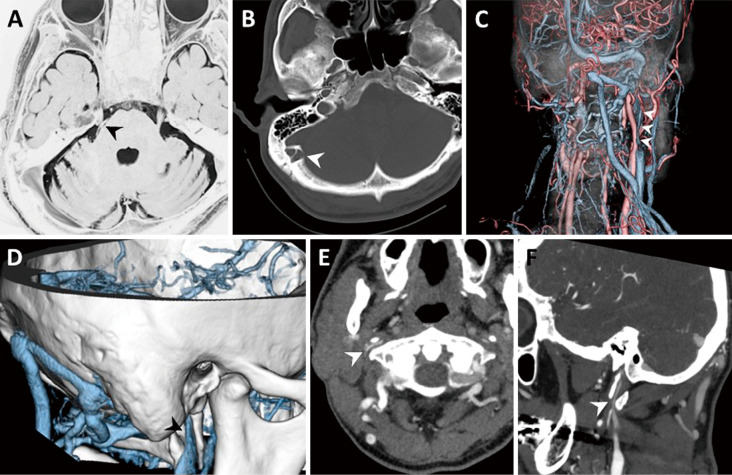
During microvascular decompression (MVD) for trigeminal neuralgia (TGN), the mastoid emissary veins (MEV) are routinely sacrificed using the suboccipital retrosigmoid approach. The technical nuances when the MEV is an important collateral venous pathway for the obstructive internal jugular vein (IJV) have not been described thus far. Herein, we demonstrate for the first time a modified surgical technique for MVD to preserve the MEV. A 62-year-old man with a 10-year history of TGN refractory to carbamazepine was referred to our hospital for MVD. Preoperative imaging revealed that the superior cerebellar artery was the offending vessel. Computed tomography angiography also revealed that his contralateral IJV pathway was hypoplastic, and the ipsilateral pathway was severely stenosed by the external compression of the elongated styloid process and the transverse process of the first cervical vertebra. The ipsilateral MEV and the connecting occipital veins were enlarged as the sole collateral pathways of intracranial venous drainage. A modified MVD technique, including an upside-down L-shaped skin incision, layer-by-layer dissection of the occipital muscles, and denuding of the intraosseous part of the MEV, was used to cure the TGN with the preservation of the venous pathway. After surgery, the pain completely diminished without any complications. In conclusion, such technical modifications would be applicable in cases where the MEV needs to be preserved during posterior fossa surgery. Preoperative screening of the venous system is also recommended.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


