Lynne Ruess, Benjamin P Thompson, Erin L Mesi, Margarita Chmil, Nicholas A Zumberge, Kari Jorgenson, Rajesh Krishnamurthy
{"title":"Increasing Engagement of Imaging Professionals in Quality Improvement Using an Encounter-specific Quality-reporting Tool.","authors":"Lynne Ruess, Benjamin P Thompson, Erin L Mesi, Margarita Chmil, Nicholas A Zumberge, Kari Jorgenson, Rajesh Krishnamurthy","doi":"10.1097/pq9.0000000000000673","DOIUrl":null,"url":null,"abstract":"<p><p>The involvement of pediatric imaging professionals in quality improvement (QI) in our department was low, with few available informatics tools to report issues or suggest improvement opportunities in a timely and efficient manner. We aimed to increase QI engagement in radiology by creating a real-time, encounter-specific reporting tool embedded into the clinical imaging workflow.</p><p><strong>Methods: </strong>A multidisciplinary team outlined requirements for a new electronic quality-reporting tool, including point-of-care access during imaging workflow and simultaneous automatic capture of encounter-specific clinical information from the hospital information system. Information system experts created a user-friendly interface for categories based on stages of imaging workflow (Planning, Acquisition, Processing, Interpretation, Communication, and Data Collection). Team members trained all department staff. Quality coordinators sorted entries and monitored personnel engagement for two 36-week periods: immediately after launch and 3 years later. Descriptive statistics were used to analyze proposed and completed QI projects during these periods.</p><p><strong>Results: </strong>There were 1,498 entries during the first 36 weeks. Ninety-three percent of radiologists and 56% of technologists participated. Three years later, there were 1,251 entries in 36 weeks. Data collection entries for established QI projects increased from 380 (25%) to 487(39%). The engagement continued among radiologists but decreased among technologists over time. Submissions for QI projects increased from baseline. The project completion rate increased.</p><p><strong>Conclusion: </strong>We created a QI reporting tool embedded into the clinical imaging workflow, which improved the participation of our imaging professionals and increased the number of completed QI projects.</p>","PeriodicalId":74412,"journal":{"name":"Pediatric quality & safety","volume":"8 4","pages":"e673"},"PeriodicalIF":1.1000,"publicationDate":"2023-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/10/91/pqs-8-e673.PMC10402949.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric quality & safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/pq9.0000000000000673","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 1
Abstract
The involvement of pediatric imaging professionals in quality improvement (QI) in our department was low, with few available informatics tools to report issues or suggest improvement opportunities in a timely and efficient manner. We aimed to increase QI engagement in radiology by creating a real-time, encounter-specific reporting tool embedded into the clinical imaging workflow.
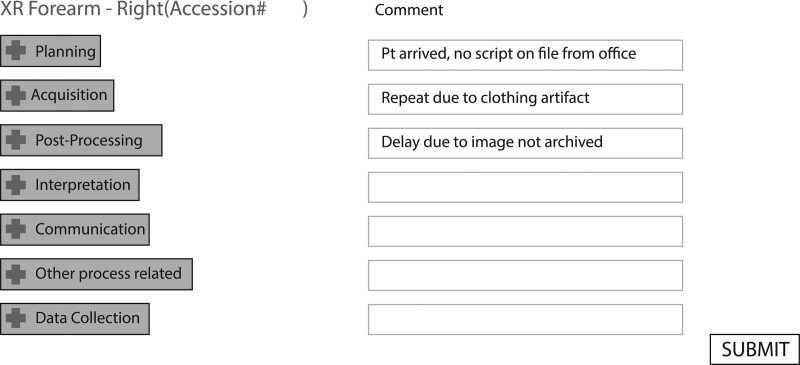
Methods: A multidisciplinary team outlined requirements for a new electronic quality-reporting tool, including point-of-care access during imaging workflow and simultaneous automatic capture of encounter-specific clinical information from the hospital information system. Information system experts created a user-friendly interface for categories based on stages of imaging workflow (Planning, Acquisition, Processing, Interpretation, Communication, and Data Collection). Team members trained all department staff. Quality coordinators sorted entries and monitored personnel engagement for two 36-week periods: immediately after launch and 3 years later. Descriptive statistics were used to analyze proposed and completed QI projects during these periods.
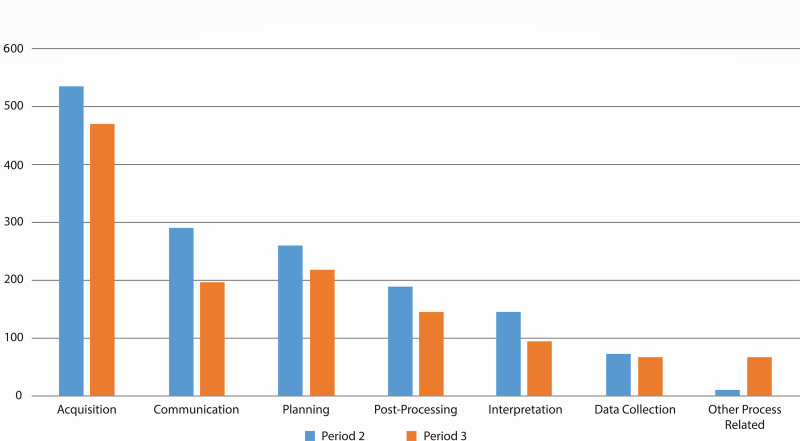
Results: There were 1,498 entries during the first 36 weeks. Ninety-three percent of radiologists and 56% of technologists participated. Three years later, there were 1,251 entries in 36 weeks. Data collection entries for established QI projects increased from 380 (25%) to 487(39%). The engagement continued among radiologists but decreased among technologists over time. Submissions for QI projects increased from baseline. The project completion rate increased.
Conclusion: We created a QI reporting tool embedded into the clinical imaging workflow, which improved the participation of our imaging professionals and increased the number of completed QI projects.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


