Yan Song, Jian-Yu E, Tracy Guo, Rahul Sasane, Steve Arcona, Nirmal Keshava, Eric Wu
{"title":"Treatment Patterns and Healthcare Resource Use in Medicare Beneficiaries with Parkinson's Disease.","authors":"Yan Song, Jian-Yu E, Tracy Guo, Rahul Sasane, Steve Arcona, Nirmal Keshava, Eric Wu","doi":"10.2147/CEOR.S422023","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Studies on real-world treatment patterns and long-term economic burden of Parkinson's disease (PD) have been limited.</p><p><strong>Objective: </strong>To assess treatment patterns, healthcare resource utilization (HRU), and costs associated with PD symptoms and treatment-related adverse events (AEs) among Medicare beneficiaries in the United States.</p><p><strong>Methods: </strong>A 100% Medicare Fee-For-Service data (2006-2020) of patients with PD were analyzed. PD treatment patterns were described for the subset of patients who had no previously observed PD treatments or diagnoses (ie, the incident cohort). HRU and healthcare costs associated with PD symptoms were assessed for all patients with PD (ie, the overall cohort) and that associated with treatment-related AEs were assessed for the subset of patients who received PD treatments after PD diagnosis (ie, the active treatment cohort), using longitudinal models with repeated measures.</p><p><strong>Results: </strong>Overall, 318,582 patients were included (mean age at PD diagnosis: 77.4 years; 53.3% female). Among patients in the incident cohort (N=214,829), 51.1% initiated levodopa monotherapy and 5.9% initiated dopamine agonists (DAs) monotherapy as first-line treatment. The proportion of incident patients treated with DAs and other PD therapies generally increased from post-diagnosis years 1 to 10. The median time from diagnosis to PD treatment initiation was 2.0 months; the median time to treatment discontinuation was the longest with levodopa (18.7 months), followed by DAs (9.5 months). In the overall cohort, PD symptoms, especially motor symptoms and severe motor symptoms, were associated with significantly higher rates of HRU and costs. In the active treatment cohort (N=234,298), treatment-related AEs were associated with significantly higher rates of HRU and medical costs.</p><p><strong>Conclusion: </strong>While levodopa is still the mainstay of PD management, considerable heterogeneity exists in real-world treatment patterns. Overall, PD symptoms and AEs were associated with significantly higher HRU and healthcare costs, suggesting unmet medical needs for PD treatments with better tolerability profiles.</p>","PeriodicalId":47313,"journal":{"name":"ClinicoEconomics and Outcomes Research","volume":"15 ","pages":"631-643"},"PeriodicalIF":2.1000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/88/08/ceor-15-631.PMC10404422.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ClinicoEconomics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/CEOR.S422023","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Studies on real-world treatment patterns and long-term economic burden of Parkinson's disease (PD) have been limited.
Objective: To assess treatment patterns, healthcare resource utilization (HRU), and costs associated with PD symptoms and treatment-related adverse events (AEs) among Medicare beneficiaries in the United States.
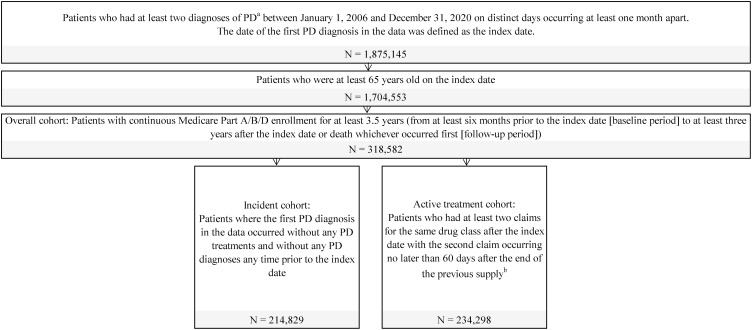
Methods: A 100% Medicare Fee-For-Service data (2006-2020) of patients with PD were analyzed. PD treatment patterns were described for the subset of patients who had no previously observed PD treatments or diagnoses (ie, the incident cohort). HRU and healthcare costs associated with PD symptoms were assessed for all patients with PD (ie, the overall cohort) and that associated with treatment-related AEs were assessed for the subset of patients who received PD treatments after PD diagnosis (ie, the active treatment cohort), using longitudinal models with repeated measures.
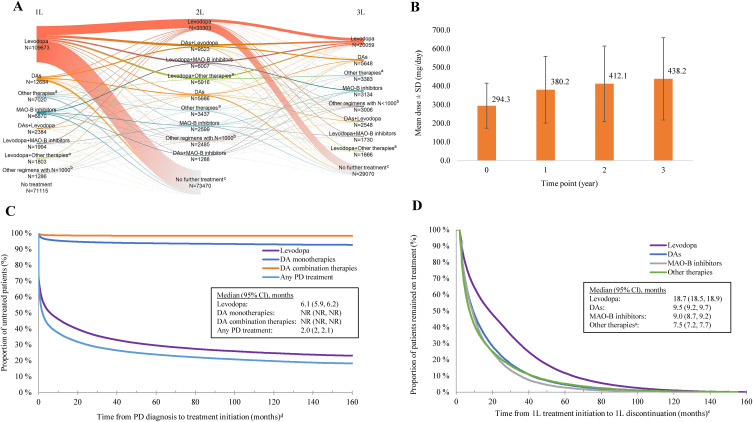
Results: Overall, 318,582 patients were included (mean age at PD diagnosis: 77.4 years; 53.3% female). Among patients in the incident cohort (N=214,829), 51.1% initiated levodopa monotherapy and 5.9% initiated dopamine agonists (DAs) monotherapy as first-line treatment. The proportion of incident patients treated with DAs and other PD therapies generally increased from post-diagnosis years 1 to 10. The median time from diagnosis to PD treatment initiation was 2.0 months; the median time to treatment discontinuation was the longest with levodopa (18.7 months), followed by DAs (9.5 months). In the overall cohort, PD symptoms, especially motor symptoms and severe motor symptoms, were associated with significantly higher rates of HRU and costs. In the active treatment cohort (N=234,298), treatment-related AEs were associated with significantly higher rates of HRU and medical costs.
Conclusion: While levodopa is still the mainstay of PD management, considerable heterogeneity exists in real-world treatment patterns. Overall, PD symptoms and AEs were associated with significantly higher HRU and healthcare costs, suggesting unmet medical needs for PD treatments with better tolerability profiles.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


