Nina M Flores, Vivian Do, Sebastian T Rowland, Joan A Casey, Marianthi A Kioumourtzoglou
{"title":"The role of insurance status in the association between short-term temperature exposure and myocardial infarction hospitalizations in New York State.","authors":"Nina M Flores, Vivian Do, Sebastian T Rowland, Joan A Casey, Marianthi A Kioumourtzoglou","doi":"10.1097/EE9.0000000000000258","DOIUrl":null,"url":null,"abstract":"<p><p>Myocardial infarction (MI) is a leading cause of morbidity and mortality in the United States and its risk increases with extreme temperatures. Climate change causes variability in weather patterns, including extreme temperature events that disproportionately affect socioeconomically disadvantaged communities. Many studies on the health effects of extreme temperatures have considered community-level socioeconomic disadvantage.</p><p><strong>Objectives: </strong>To evaluate effect modification of the relationship between short-term ambient temperature and MI, by individual-level insurance status (insured vs. uninsured).</p><p><strong>Methods: </strong>We identified MI hospitalizations and insurance status across New York State (NYS) hospitals from 1995 to 2015 in the New York Department of Health Statewide Planning and Research Cooperative System database, using <i>International Classification of Diseases</i> codes. We linked short-term ambient temperature (averaging the 6 hours preceding the event [MI hospitalization]) or nonevent control period in patient residential zip codes. We employed a time-stratified case-crossover study design for both insured and uninsured strata, and then compared the group-specific rate ratios.</p><p><strong>Results: </strong>Over the study period, there were 1,095,051 primary MI admissions, 966,475 (88%) among insured patients. During extremely cold temperatures (<5.8 °C) insured patients experienced reduced rates of MI; this was not observed among the uninsured counterparts. At warmer temperatures starting at the 65th percentile (15.7 °C), uninsured patients had higher rates than insured patients (e.g., for a 6-hour pre-event average temperature increase from the median to the 75th percentile, the rate of MI increased was 2.0% [0.0%-4.0%] higher in uninsured group).</p><p><strong>Conclusions: </strong>Uninsured individuals may face disproportionate rates of MI hospitalization during extreme temperatures.</p>","PeriodicalId":72930,"journal":{"name":"","volume":"7 4","pages":"e258"},"PeriodicalIF":0.0,"publicationDate":"2023-07-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/6e/1d/ee9-7-e258.PMC10403039.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/EE9.0000000000000258","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/8/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Myocardial infarction (MI) is a leading cause of morbidity and mortality in the United States and its risk increases with extreme temperatures. Climate change causes variability in weather patterns, including extreme temperature events that disproportionately affect socioeconomically disadvantaged communities. Many studies on the health effects of extreme temperatures have considered community-level socioeconomic disadvantage.
Objectives: To evaluate effect modification of the relationship between short-term ambient temperature and MI, by individual-level insurance status (insured vs. uninsured).
Methods: We identified MI hospitalizations and insurance status across New York State (NYS) hospitals from 1995 to 2015 in the New York Department of Health Statewide Planning and Research Cooperative System database, using International Classification of Diseases codes. We linked short-term ambient temperature (averaging the 6 hours preceding the event [MI hospitalization]) or nonevent control period in patient residential zip codes. We employed a time-stratified case-crossover study design for both insured and uninsured strata, and then compared the group-specific rate ratios.
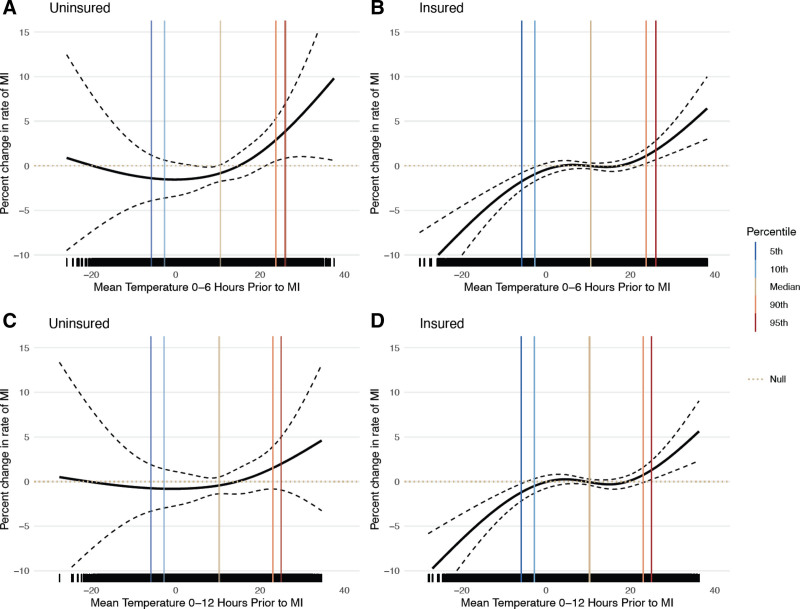
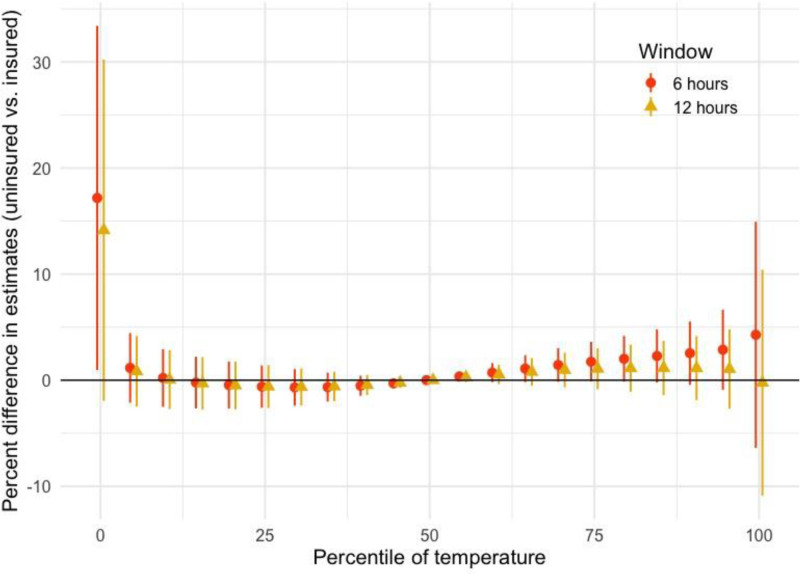
Results: Over the study period, there were 1,095,051 primary MI admissions, 966,475 (88%) among insured patients. During extremely cold temperatures (<5.8 °C) insured patients experienced reduced rates of MI; this was not observed among the uninsured counterparts. At warmer temperatures starting at the 65th percentile (15.7 °C), uninsured patients had higher rates than insured patients (e.g., for a 6-hour pre-event average temperature increase from the median to the 75th percentile, the rate of MI increased was 2.0% [0.0%-4.0%] higher in uninsured group).
Conclusions: Uninsured individuals may face disproportionate rates of MI hospitalization during extreme temperatures.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


