Management of anastomotic leakage after robot-assisted minimally invasive esophagectomy with an intrathoracic anastomosis.
Diseases of the esophagus : official journal of the International Society for Diseases of the Esophagus
Pub Date : 2023-05-27
DOI:10.1093/dote/doac094
引用次数: 0
Abstract
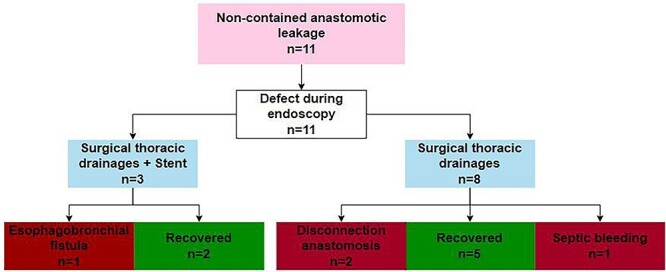
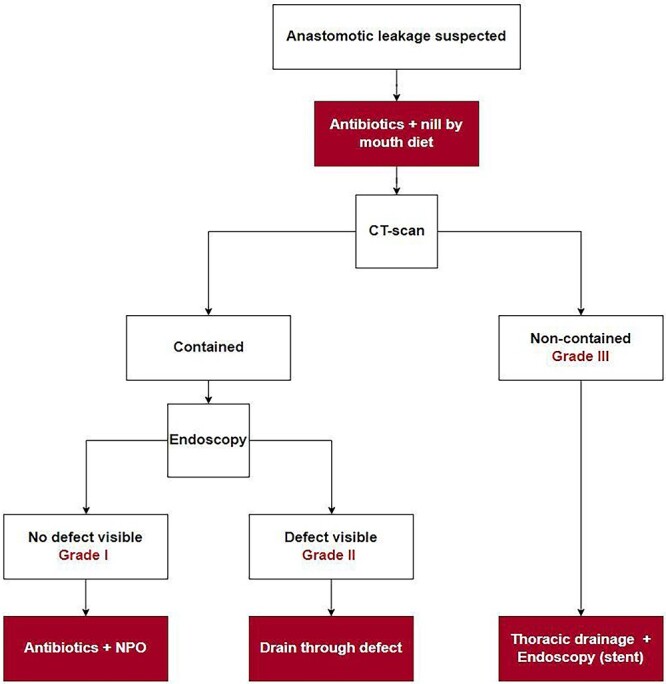
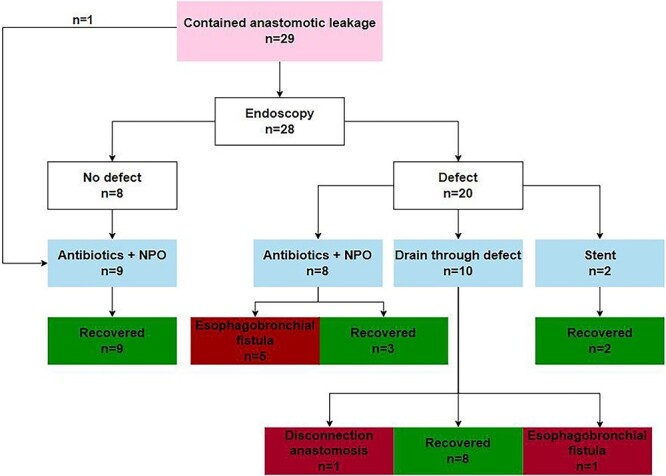
Abstract Anastomotic leakage is a feared complication after esophagectomy and associated with increased post-operative morbidity and mrotality. The aim of this study was to evaluate the management of leakage after robot-assisted minimally invasive esophagectomy (RAMIE) with intrathoracic anastomosis. From a single center prospectively maintained database, all patients with anastomotic leakages defined by the Esophageal Complications Consensus Group between 2016 and 2021 were included. Contained leakage was defined as presence of air or fluid at level of the anastomosis without the involvement of the mediastinum or thorax. Non-contained leakage was defined as mediastinitis and/or mediastinal/pleural fluid collections. The primary outcome was 90-day mortality and the secondary outcome was successful recovery. In this study, 40 patients with anastomotic leakage were included. The 90-day mortality rate was 3% (n = 1). Leakage was considered contained in 29 patients (73%) and non-contained in 11 patients (27%). In the contained group, the majority of the patients were treated non-surgically (n = 27, 93%) and management was successful in 22 patients (76%). In the non-contained group, all patients required a reoperation with thoracic drainage and management was successful in seven patients (64%). Management failed in 11 patients (28%) of whom 7 developed an esophagobronchial fistula, 3 had a disconnection of the anastomosis and 1 died of a septic bleeding. In conclusion, this study demonstrates that the management anastomotic leakage in patients who underwent RAMIE with an intrathoracic anastomosis was successful in 73% of the patients with a 90-day mortality rate of 3%. A differentiated approach for the management of intrathoracic anastomotic leakage is proposed.
机器人辅助微创食管切除术胸内吻合术后吻合口瘘的处理。
吻合口漏是食管切除术后令人担忧的并发症,并与术后发病率和死亡率增加有关。本研究的目的是评估机器人辅助微创食管切除术(RAMIE)胸内吻合术后渗漏的处理。从一个单中心前瞻性维护的数据库中,纳入了2016年至2021年间食管并发症共识组定义的所有吻合口瘘患者。包含性渗漏定义为在吻合处存在空气或液体,但未累及纵隔或胸腔。非控制性渗漏被定义为纵隔炎和/或纵隔/胸腔积液。主要终点为90天死亡率,次要终点为成功恢复。本研究纳入了40例吻合口瘘患者。90天死亡率为3% (n = 1)。29例(73%)患者认为渗漏得到控制,11例(27%)患者认为渗漏未得到控制。在对照组中,大多数患者采用非手术治疗(n = 27, 93%), 22例(76%)患者治疗成功。在非封闭组中,所有患者都需要再次手术并进行胸腔引流,7例患者(64%)成功处理。11例(28%)患者治疗失败,其中7例发生食管支气管瘘,3例吻合口断开,1例死于脓毒性出血。总之,本研究表明,73%的RAMIE胸内吻合患者成功处理吻合口漏,90天死亡率为3%。提出了一种治疗胸内吻合口瘘的鉴别方法。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊

自引率
0.00%
发文量
0
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


