{"title":"Isolated Oculomotor Nerve Palsy after Mechanical Thrombectomy for Middle Cerebral Artery Occlusion: A Case Report.","authors":"Hidefumi Amisaki, Hirochika Takeuchi, Makoto Sakamoto, Hisashi Shishido","doi":"10.5797/jnet.cr.2022-0070","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Complications of mechanical thrombectomy (MT) should be identified and managed because they often worsen clinical outcomes. Here we present a case of post-MT embolization of the artery supplying the oculomotor nerve, which has not previously been reported as a complication of MT.</p><p><strong>Case presentation: </strong>An 81-year-old woman visited our hospital within 2 hours of the sudden onset of left hemiparesis and impaired awareness. MRA showed right middle cerebral artery (MCA) M1 segment occlusion and a possibly salvageable penumbra. We performed thrombectomy for right MCA occlusion with successful recanalization. In the final angiography view, the marginal tentorial artery was almost invisible. Ten hours after thrombectomy, the patient developed complete right oculomotor nerve palsy. Subsequent MRI showed ischemic lesions, but none in the oculomotor nucleus, and there were no lesions compressing the oculomotor nerve. We presume that embolization of the marginal tentorial artery caused oculomotor nerve palsy. The intracranial middle and distal portions of the oculomotor nerve are supplied by the superior branches of the inferolateral trunk and by the marginal tentorial artery.</p><p><strong>Conclusion: </strong>Occlusion of the marginal tentorial artery can cause oculomotor nerve palsy, although this has not previously been reported. Our case suggests that neurointerventional surgeons should evaluate patency of branches of the inferolateral trunk and the meningohypophyseal trunk during the procedure of MT.</p>","PeriodicalId":73856,"journal":{"name":"Journal of neuroendovascular therapy","volume":"17 4","pages":"97-100"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/0b/2c/jnet-17-97.PMC10370629.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of neuroendovascular therapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5797/jnet.cr.2022-0070","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Complications of mechanical thrombectomy (MT) should be identified and managed because they often worsen clinical outcomes. Here we present a case of post-MT embolization of the artery supplying the oculomotor nerve, which has not previously been reported as a complication of MT.
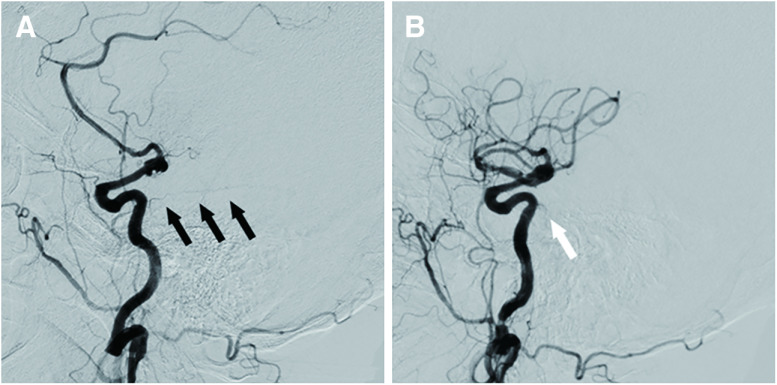
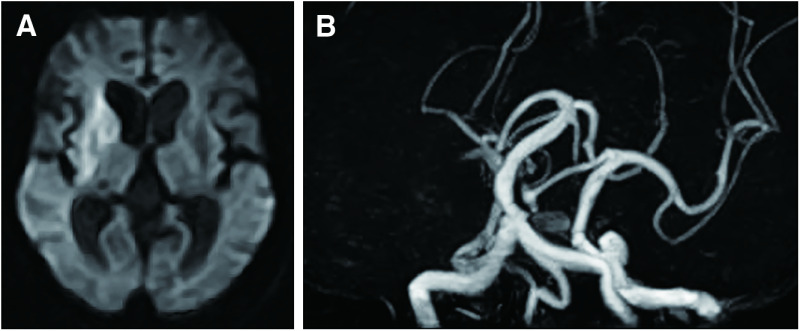
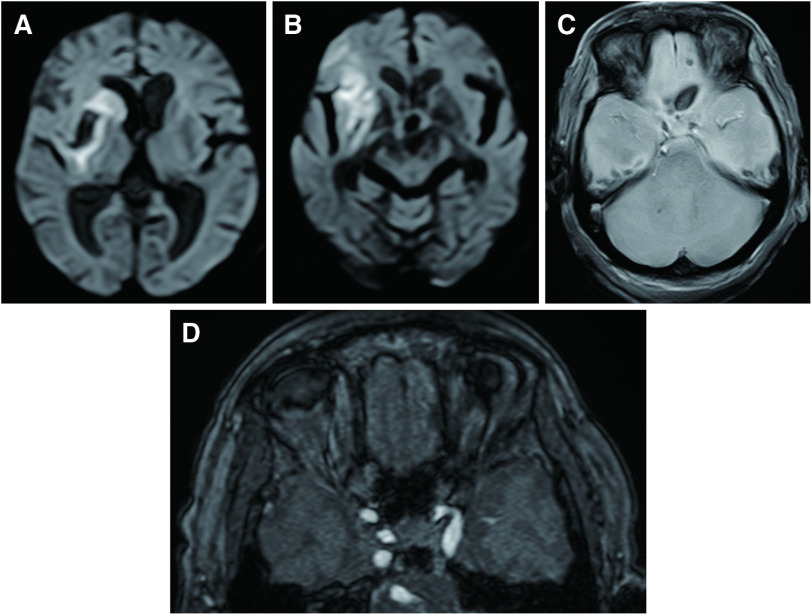
Case presentation: An 81-year-old woman visited our hospital within 2 hours of the sudden onset of left hemiparesis and impaired awareness. MRA showed right middle cerebral artery (MCA) M1 segment occlusion and a possibly salvageable penumbra. We performed thrombectomy for right MCA occlusion with successful recanalization. In the final angiography view, the marginal tentorial artery was almost invisible. Ten hours after thrombectomy, the patient developed complete right oculomotor nerve palsy. Subsequent MRI showed ischemic lesions, but none in the oculomotor nucleus, and there were no lesions compressing the oculomotor nerve. We presume that embolization of the marginal tentorial artery caused oculomotor nerve palsy. The intracranial middle and distal portions of the oculomotor nerve are supplied by the superior branches of the inferolateral trunk and by the marginal tentorial artery.
Conclusion: Occlusion of the marginal tentorial artery can cause oculomotor nerve palsy, although this has not previously been reported. Our case suggests that neurointerventional surgeons should evaluate patency of branches of the inferolateral trunk and the meningohypophyseal trunk during the procedure of MT.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


