{"title":"Digoxin for the Management of Unstable Paroxysmal Supraventricular Tachycardia in a Patient Who Refused Electrical Cardioversion in a Rural Hospital.","authors":"Belayneh Dessie Kassa, Mekbib Amede, Mollalign Wubante, Mebratu Libanos, Kumlachew Geta","doi":"10.1155/2023/7301460","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The most frequent atrioventricular tachycardia in the emergency room is atrioventricular nodal reentrant tachycardia (AVNRT). The first treatment option for ending stable narrow QRS complex SVTs is vagal maneuvers and adenosine. When adenosine or vagal maneuvers fail to change a patient's rhythm to normal sinus rhythm, long-acting AV nodal-blocking medications, including nondihydropyridine calcium channel blockers (verapamil and diltiazem), flecainide, or beta-blockers, are employed. Electricity (synchronized cardioversion) is the preferred form of treatment for unstable patients. <i>Case Presentation</i>. A 40-year-old male patient presented to the Emergency Department of Dubti General Hospital, the Afar regional state in Ethiopia, with a complaint of shortness of breath, palpitation, extreme fatigue, and chest pain of a day's duration. His blood pressure was 80/50 mmHg, he had cold extremities and a weak radial pulse, and his apical heart rate was fast, making it difficult to count. His electrocardiogram (ECG) showed paroxysmal supraventricular tachycardia (PSVT) with a heart rate of 200. He was a candidate for electrical cardioversion due to unstable PSVT, but he and his family members refused to give consent. Even though he is not indicated for pharmacologic therapy, none of the commonly used drugs were available at the hospital. We managed him with digoxin, and the outcome was positive.</p><p><strong>Conclusion: </strong>Even though we could not find a clear recommendation regarding the use of digoxin for patients with unstable PSVT (AVNRT), by taking into consideration its negative chronotropic effect and its action to suppress the AV nodal conduction velocity, it may reduce the heart rate, and it can be used as an alternative in such difficult scenarios and a resource-limited setting. But this should be further investigated.</p>","PeriodicalId":9624,"journal":{"name":"Case Reports in Emergency Medicine","volume":"2023 ","pages":"7301460"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10344630/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2023/7301460","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
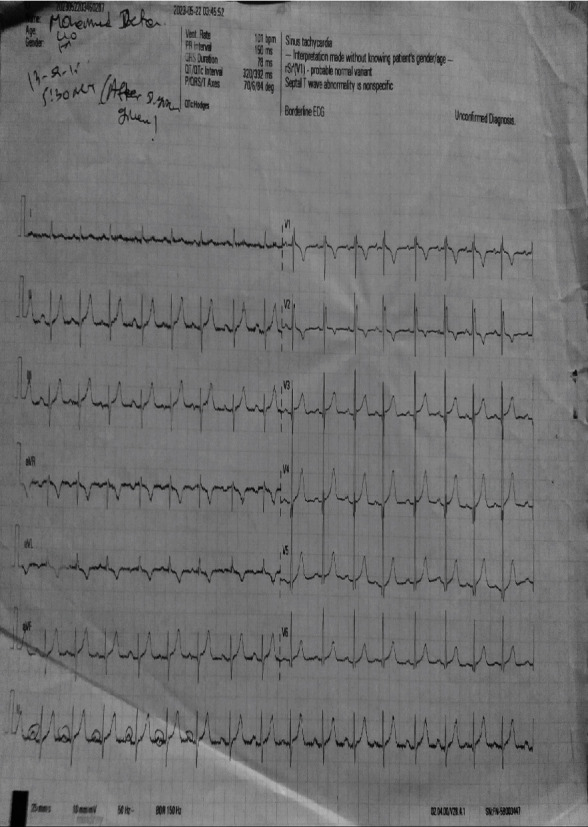
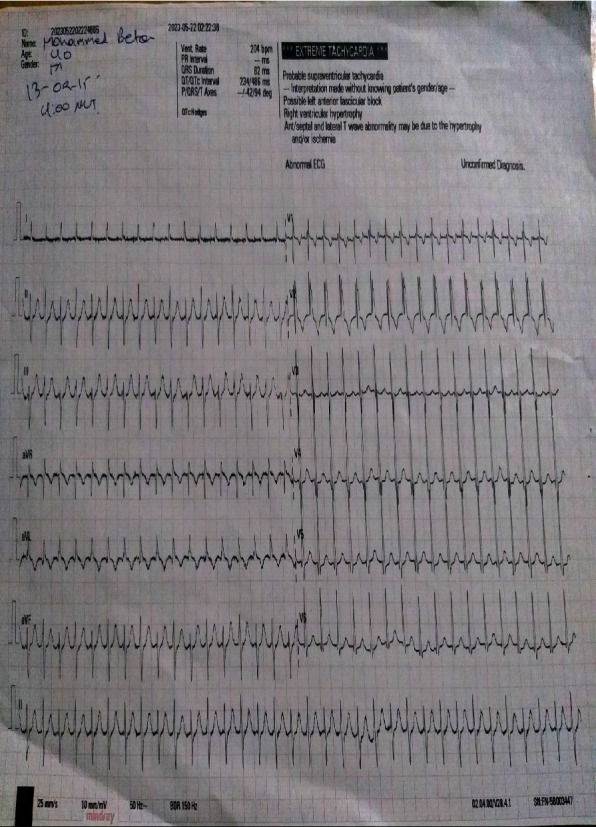
Background: The most frequent atrioventricular tachycardia in the emergency room is atrioventricular nodal reentrant tachycardia (AVNRT). The first treatment option for ending stable narrow QRS complex SVTs is vagal maneuvers and adenosine. When adenosine or vagal maneuvers fail to change a patient's rhythm to normal sinus rhythm, long-acting AV nodal-blocking medications, including nondihydropyridine calcium channel blockers (verapamil and diltiazem), flecainide, or beta-blockers, are employed. Electricity (synchronized cardioversion) is the preferred form of treatment for unstable patients. Case Presentation. A 40-year-old male patient presented to the Emergency Department of Dubti General Hospital, the Afar regional state in Ethiopia, with a complaint of shortness of breath, palpitation, extreme fatigue, and chest pain of a day's duration. His blood pressure was 80/50 mmHg, he had cold extremities and a weak radial pulse, and his apical heart rate was fast, making it difficult to count. His electrocardiogram (ECG) showed paroxysmal supraventricular tachycardia (PSVT) with a heart rate of 200. He was a candidate for electrical cardioversion due to unstable PSVT, but he and his family members refused to give consent. Even though he is not indicated for pharmacologic therapy, none of the commonly used drugs were available at the hospital. We managed him with digoxin, and the outcome was positive.
Conclusion: Even though we could not find a clear recommendation regarding the use of digoxin for patients with unstable PSVT (AVNRT), by taking into consideration its negative chronotropic effect and its action to suppress the AV nodal conduction velocity, it may reduce the heart rate, and it can be used as an alternative in such difficult scenarios and a resource-limited setting. But this should be further investigated.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


