Benjamin J Worrall, Alexander Papachristos, Ahmad Aniss, Anthony Glover, Stan B Sidhu, Roderick J Clifton-Bligh, Diana Learoyd, Venessa H M Tsang, Matti Gild, Bruce G Robinson, Mark S Sywak
{"title":"Lobectomy and completion thyroidectomy rates increase after the 2015 American Thyroid Association Differentiated Thyroid Cancer Guidelines update.","authors":"Benjamin J Worrall, Alexander Papachristos, Ahmad Aniss, Anthony Glover, Stan B Sidhu, Roderick J Clifton-Bligh, Diana Learoyd, Venessa H M Tsang, Matti Gild, Bruce G Robinson, Mark S Sywak","doi":"10.1530/EO-22-0095","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The 2015 American Thyroid Association (ATA) Guidelines permit thyroid lobectomy (TL) or total thyroidectomy in the management of low-risk papillary thyroid cancer (PTC). As definitive risk-stratification is only possible post-operatively, some patients may require completion thyroidectomy (CT) after final histopathological analysis.</p><p><strong>Methods: </strong>A retrospective cohort study of patients undergoing surgery for low-risk PTC in a tertiary referral centre was undertaken. Consecutive adult patients treated from January 2013 to March 2021 were divided into two groups (pre- and post-publication of ATA Guidelines on 01/01/2016). Only those eligible for lobectomy under rule 35(B) of the ATA Guidelines were included: Bethesda V/VI cytology, 1-4 cm post-operative size and without pre-operative evidence of extrathyroidal extension or nodal metastases. We examined rates of TL, CT, local recurrence and surgical complications.</p><p><strong>Results: </strong>There were 1488 primary surgical procedures performed for PTC on consecutive adult patients during the study period, of which 461 were eligible for TL. Mean tumour size (<i>P</i> = 0.20) and mean age (<i>P</i> = 0.78) were similar between time periods. The TL rate increased significantly from 4.5 to 18% in the post-publication period (<i>P</i> < 0.001). The proportion of TL patients requiring CT (43 vs 38%) was similar between groups (<i>P</i> = 1.0). There was no significant change in complications (<i>P</i> = 0.55) or local recurrence rates (<i>P</i> = 0.24).</p><p><strong>Conclusion: </strong>The introduction of the 2015 ATA Guidelines resulted in a modest but significant increase in the rate of lobectomy for eligible PTC patients. In the post-publication period, 38% of patients who underwent TL ultimately required CT after complete pathological analysis.</p>","PeriodicalId":72907,"journal":{"name":"Endocrine oncology (Bristol, England)","volume":"3 1","pages":"e220095"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/9f/ba/EO-22-0095.PMC10305631.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Endocrine oncology (Bristol, England)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1530/EO-22-0095","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The 2015 American Thyroid Association (ATA) Guidelines permit thyroid lobectomy (TL) or total thyroidectomy in the management of low-risk papillary thyroid cancer (PTC). As definitive risk-stratification is only possible post-operatively, some patients may require completion thyroidectomy (CT) after final histopathological analysis.
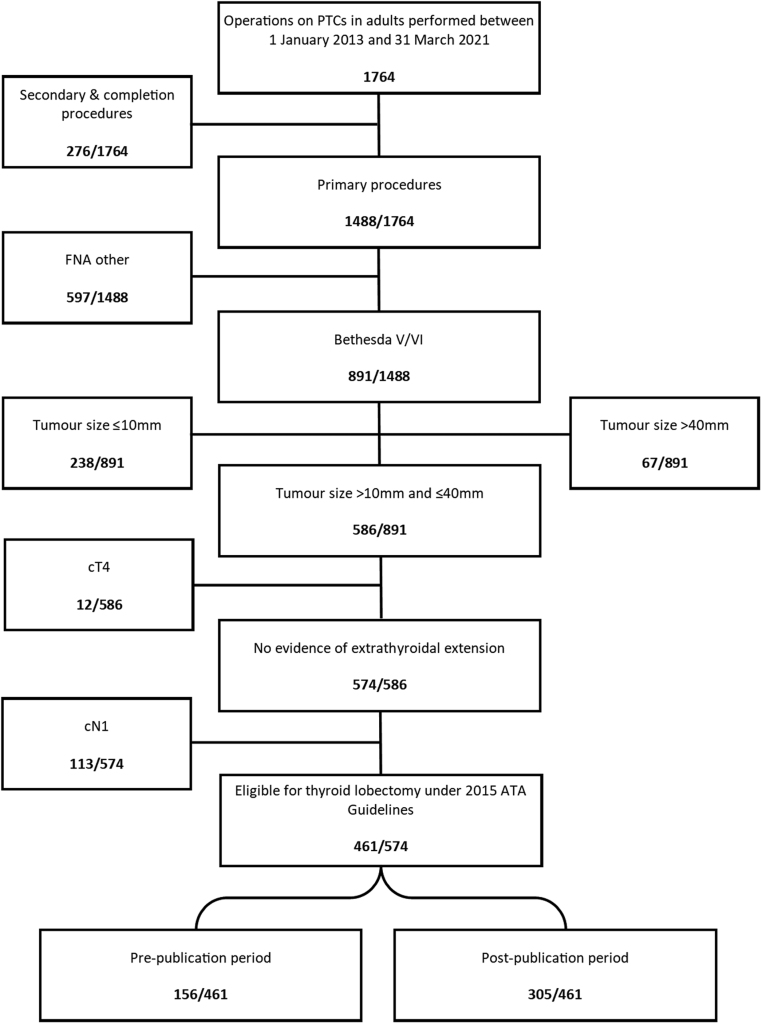
Methods: A retrospective cohort study of patients undergoing surgery for low-risk PTC in a tertiary referral centre was undertaken. Consecutive adult patients treated from January 2013 to March 2021 were divided into two groups (pre- and post-publication of ATA Guidelines on 01/01/2016). Only those eligible for lobectomy under rule 35(B) of the ATA Guidelines were included: Bethesda V/VI cytology, 1-4 cm post-operative size and without pre-operative evidence of extrathyroidal extension or nodal metastases. We examined rates of TL, CT, local recurrence and surgical complications.
Results: There were 1488 primary surgical procedures performed for PTC on consecutive adult patients during the study period, of which 461 were eligible for TL. Mean tumour size (P = 0.20) and mean age (P = 0.78) were similar between time periods. The TL rate increased significantly from 4.5 to 18% in the post-publication period (P < 0.001). The proportion of TL patients requiring CT (43 vs 38%) was similar between groups (P = 1.0). There was no significant change in complications (P = 0.55) or local recurrence rates (P = 0.24).
Conclusion: The introduction of the 2015 ATA Guidelines resulted in a modest but significant increase in the rate of lobectomy for eligible PTC patients. In the post-publication period, 38% of patients who underwent TL ultimately required CT after complete pathological analysis.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


