Single-Dose Pharmacokinetics and Total Removal of Cyclophosphamide in a Patient with Acute Kidney Injury Undergoing Intermittent Haemodialysis and Prolonged Intermittent Kidney Replacement Therapy: A Case Report.
Catherina Lück, Gernot Beutel, W Nikolaus Kühn-Velten, Jan T Kielstein
{"title":"Single-Dose Pharmacokinetics and Total Removal of Cyclophosphamide in a Patient with Acute Kidney Injury Undergoing Intermittent Haemodialysis and Prolonged Intermittent Kidney Replacement Therapy: A Case Report.","authors":"Catherina Lück, Gernot Beutel, W Nikolaus Kühn-Velten, Jan T Kielstein","doi":"10.1159/000531129","DOIUrl":null,"url":null,"abstract":"<p><p>The largest study on cyclophosphamide pharmacokinetics in dialysis patients comprises of 6 subjects. In the 2 decades since these data were obtained, dialyser membranes, treatment intensities, and treatment duration have changed considerably making new pharmacokinetic studies desirable. We aimed to readdress the pharmacokinetics of cyclophosphamide in a 74-year-old critically ill male suffering from ANCA-associated vasculitis. Due to an acute-on-chronic kidney injury, he underwent intermittent (IHD) and prolonged intermittent kidney replacement therapy (PIKRT). IHD was started 7 h after end of a cyclophosphamide infusion with a blood/dialysate flow of 300 mL/min for 255 min, followed by PIKRT with a blood/dialysate flow of 140 mL/min for 540 min, both using a 1.3 m<sup>2</sup> polysulphone high-flux dialyser (F60S, Fresenius Medical Care). Peak concentration of cyclophosphamide was 20.2 mg/L. Using IHD and PIKRT serum concentration of cyclophosphamide decreased to 1.2 mg/L after IHD and to <0.1 mg/L after PIKRT with dialyser-clearances of 153.0 mL/min and 84.9 mL/min, respectively. Total recovery of cyclophosphamide, calculated from the collected dialysate, was 57.5 mg (7.7% of administered dose) for IHD and was 8.3 mg (1.1% of administered dose) for PIKRT. By using IHD with a high-flux dialyser cyclophosphamide could be eliminated. Remaining cyclophosphamide should be eliminated by PIKRT. Hence, even in the absence of renal function a dose >50% of the recommended for patient with normal renal function may be applied, as complete elimination of the parent drug by modern dialysis is feasible.</p>","PeriodicalId":9599,"journal":{"name":"Case Reports in Nephrology and Dialysis","volume":"13 1","pages":"70-74"},"PeriodicalIF":0.9000,"publicationDate":"2023-07-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/06/5f/cnd-2023-0013-0001-531129.PMC10359690.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Nephrology and Dialysis","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000531129","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
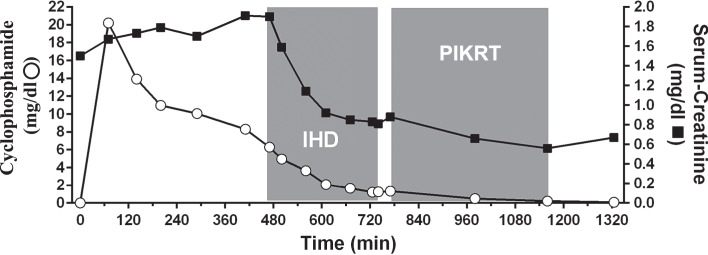
The largest study on cyclophosphamide pharmacokinetics in dialysis patients comprises of 6 subjects. In the 2 decades since these data were obtained, dialyser membranes, treatment intensities, and treatment duration have changed considerably making new pharmacokinetic studies desirable. We aimed to readdress the pharmacokinetics of cyclophosphamide in a 74-year-old critically ill male suffering from ANCA-associated vasculitis. Due to an acute-on-chronic kidney injury, he underwent intermittent (IHD) and prolonged intermittent kidney replacement therapy (PIKRT). IHD was started 7 h after end of a cyclophosphamide infusion with a blood/dialysate flow of 300 mL/min for 255 min, followed by PIKRT with a blood/dialysate flow of 140 mL/min for 540 min, both using a 1.3 m2 polysulphone high-flux dialyser (F60S, Fresenius Medical Care). Peak concentration of cyclophosphamide was 20.2 mg/L. Using IHD and PIKRT serum concentration of cyclophosphamide decreased to 1.2 mg/L after IHD and to <0.1 mg/L after PIKRT with dialyser-clearances of 153.0 mL/min and 84.9 mL/min, respectively. Total recovery of cyclophosphamide, calculated from the collected dialysate, was 57.5 mg (7.7% of administered dose) for IHD and was 8.3 mg (1.1% of administered dose) for PIKRT. By using IHD with a high-flux dialyser cyclophosphamide could be eliminated. Remaining cyclophosphamide should be eliminated by PIKRT. Hence, even in the absence of renal function a dose >50% of the recommended for patient with normal renal function may be applied, as complete elimination of the parent drug by modern dialysis is feasible.
期刊介绍:
This peer-reviewed online-only journal publishes original case reports covering the entire spectrum of nephrology and dialysis, including genetic susceptibility, clinical presentation, diagnosis, treatment or prevention, toxicities of therapy, critical care, supportive care, quality-of-life and survival issues. The journal will also accept case reports dealing with the use of novel technologies, both in the arena of diagnosis and treatment. Supplementary material is welcomed.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


