A Nomogram for Identifying HR+/Her2- Breast Cancer Patients with Positive Sentinel Lymph Nodes and Omitted Axillary Lymph Node Dissection Who Need Abemaciclib Therapy.
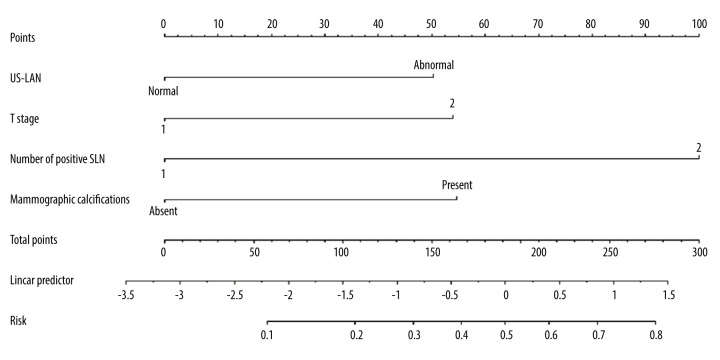
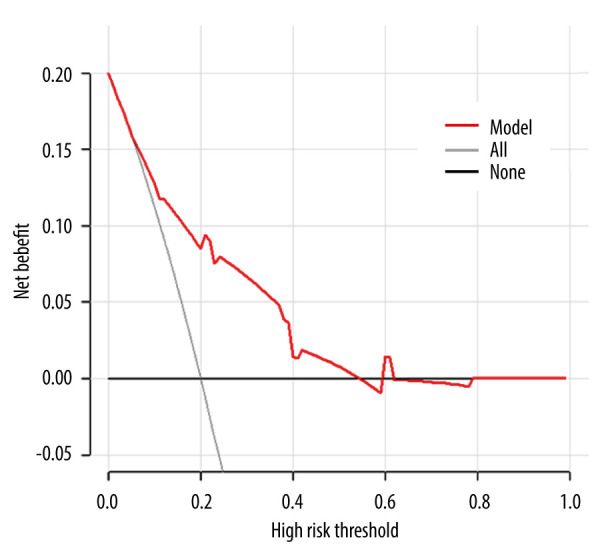
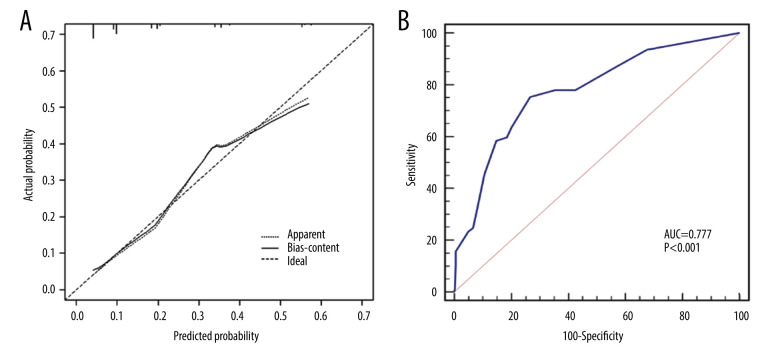
{"title":"A Nomogram for Identifying HR+/Her2- Breast Cancer Patients with Positive Sentinel Lymph Nodes and Omitted Axillary Lymph Node Dissection Who Need Abemaciclib Therapy.","authors":"Hanzhao Yang, Yadong Sun, Peili Wang, Jianghua Qiao, Lianfang Li, Zhenduo Lu, Xianfu Sun, Chongjian Zhang, Xiuchun Chen, Min Yan, Shude Cui, Chengzheng Wang, Zhenzhen Liu","doi":"10.12659/MSM.940124","DOIUrl":null,"url":null,"abstract":"<p><p>BACKGROUND The efficacy of abemaciclib in high-risk patients with early-stage HR+/Her2- breast cancer has been verified by MonarchE. However, accurately determining the number of axillary lymph node (ALN) metastases remains challenging. The Z0011 trial changed the axillary management strategy, eliminating the need for axillary lymph node dissection (ALND) in patients with 1-2 sentinel lymph node (SLN) metastases. Therefore, further exploration is needed to identify patients who could benefit from abemaciclib therapy. MATERIAL AND METHODS This retrospective study included cT1-2N0M0 HR+/Her2- patients with 1-2 positive SLNs who underwent ALND. Clinicopathological data were collected, and logistic regression analyses identified independent predictors for ≥4 positive ALNs. A predictive nomogram was developed, and discrimination and calibration were evaluated using the C-index and calibration curve. Clinical efficacy was assessed using decision curve analysis (DCA). RESULTS We enrolled 444 patients, with 77 (17.3%) having ≥4 positive ALNs. Independent predictors for ≥4 positive ALNs included abnormal ALN on ultrasound, mammographic calcifications, T stage, and the number of positive SLNs. The nomogram demonstrated an AUC of 0.777 (95% CI: 0.735-0.815, P<0.001), and internal validation showed good calibration and discrimination (C-index, 0.802; 95% CI: 0.779-0.824). DCA revealed a positive net benefit for risk levels ranging from 5% to 54%. CONCLUSIONS This nomogram is a convenient and reliable tool to predict the risk of ≥4 positive ALNs in HR+/Her2- patients. It aids in protocol selection by identifying SLN-positive patients who may benefit from abemaciclib therapy without ALND.</p>","PeriodicalId":18276,"journal":{"name":"Medical Science Monitor : International Medical Journal of Experimental and Clinical Research","volume":"29 ","pages":"e940124"},"PeriodicalIF":0.0000,"publicationDate":"2023-07-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c7/7a/medscimonit-29-e940124.PMC10357967.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medical Science Monitor : International Medical Journal of Experimental and Clinical Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.12659/MSM.940124","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
BACKGROUND The efficacy of abemaciclib in high-risk patients with early-stage HR+/Her2- breast cancer has been verified by MonarchE. However, accurately determining the number of axillary lymph node (ALN) metastases remains challenging. The Z0011 trial changed the axillary management strategy, eliminating the need for axillary lymph node dissection (ALND) in patients with 1-2 sentinel lymph node (SLN) metastases. Therefore, further exploration is needed to identify patients who could benefit from abemaciclib therapy. MATERIAL AND METHODS This retrospective study included cT1-2N0M0 HR+/Her2- patients with 1-2 positive SLNs who underwent ALND. Clinicopathological data were collected, and logistic regression analyses identified independent predictors for ≥4 positive ALNs. A predictive nomogram was developed, and discrimination and calibration were evaluated using the C-index and calibration curve. Clinical efficacy was assessed using decision curve analysis (DCA). RESULTS We enrolled 444 patients, with 77 (17.3%) having ≥4 positive ALNs. Independent predictors for ≥4 positive ALNs included abnormal ALN on ultrasound, mammographic calcifications, T stage, and the number of positive SLNs. The nomogram demonstrated an AUC of 0.777 (95% CI: 0.735-0.815, P<0.001), and internal validation showed good calibration and discrimination (C-index, 0.802; 95% CI: 0.779-0.824). DCA revealed a positive net benefit for risk levels ranging from 5% to 54%. CONCLUSIONS This nomogram is a convenient and reliable tool to predict the risk of ≥4 positive ALNs in HR+/Her2- patients. It aids in protocol selection by identifying SLN-positive patients who may benefit from abemaciclib therapy without ALND.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


