Randomised study of bailout intracranial angioplasty following thrombectomy for acute large vessel occlusion (ANGEL-REBOOT): protocol of a multicentre randomised controlled trial.
Feng Gao, Xu Tong, Baixue Jia, Ming Yang, Yuesong Pan, Zeguang Ren, William Scott Burgin, Liping Liu, Xingquan Zhao, Yilong Wang, Yongjun Wang, Zhongrong Miao
{"title":"Randomised study of bailout intracranial angioplasty following thrombectomy for acute large vessel occlusion (ANGEL-REBOOT): protocol of a multicentre randomised controlled trial.","authors":"Feng Gao, Xu Tong, Baixue Jia, Ming Yang, Yuesong Pan, Zeguang Ren, William Scott Burgin, Liping Liu, Xingquan Zhao, Yilong Wang, Yongjun Wang, Zhongrong Miao","doi":"10.1136/svn-2023-002433","DOIUrl":null,"url":null,"abstract":"<p><strong>Rationale: </strong>Unsuccessful thrombectomy of acute large vessel occlusions (LVOs) has been associated with unfavourable outcomes. Multiple randomised controlled trials (RCTs) have reported a failure rate of 12%-41% for thrombectomy procedures. Various factors contribute to failed thrombectomy, including technical difficulties in accessing the occlusion, unsuccessful thrombus retrieval, thrombotic reocclusion and pre-existing intracranial atherosclerotic stenosis. Although some studies have explored balloon dilation or permanent stenting as rescue intracranial angioplasty for failed thrombectomy in individual cases, there is currently no evidence from RCTs on this specific topic.</p><p><strong>Aim: </strong>To evaluate the potential superiority of bailout angioplasty over standard treatment in cases of unsuccessful recanalisation (eTICI 0 to 2a) or residual severe stenosis (>70%) after thrombectomy in acute LVO patients within 24 hours of stroke onset.</p><p><strong>Design: </strong>This study is a multicentre, prospective, randomised, controlled clinical trial designed by investigators. It compares bailout angioplasty with standard therapy and follows an open-label treatment approach while maintaining a blinded outcome assessment (PROBE design). Our objective is to allocate 348 patients in a 1:1 ratio to either receive bailout angioplasty as an intervention or standard therapy as a control, following unsuccessful thrombectomy.</p><p><strong>Outcome: </strong>The main measure of interest is the modified Rankin Scale (mRS) Score, which will be assessed in a blinded manner at 90 (±14) days following randomisation. The primary effect size will be determined using ordered logistic regression to calculate the common OR, representing the shift on the six-category mRS Scale at the 90-day mark. Additionally, the safety outcomes will be evaluated, including symptomatic intracranial haemorrhage within 18-36 hours, severe procedure-related complications and mortality within 90 (±14) days, among others.</p><p><strong>Discussion: </strong>The ANGEL-REBOOT study aims to generate substantial evidence regarding the efficacy and safety of bailout intracranial angioplasty as a treatment option for patients with LVO who have experienced unsuccessful thrombectomy.</p><p><strong>Trial registration number: </strong>NCT05122286.</p>","PeriodicalId":22021,"journal":{"name":"Stroke and Vascular Neurology","volume":" ","pages":"181-188"},"PeriodicalIF":4.9000,"publicationDate":"2024-04-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11103159/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Stroke and Vascular Neurology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/svn-2023-002433","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Rationale: Unsuccessful thrombectomy of acute large vessel occlusions (LVOs) has been associated with unfavourable outcomes. Multiple randomised controlled trials (RCTs) have reported a failure rate of 12%-41% for thrombectomy procedures. Various factors contribute to failed thrombectomy, including technical difficulties in accessing the occlusion, unsuccessful thrombus retrieval, thrombotic reocclusion and pre-existing intracranial atherosclerotic stenosis. Although some studies have explored balloon dilation or permanent stenting as rescue intracranial angioplasty for failed thrombectomy in individual cases, there is currently no evidence from RCTs on this specific topic.
Aim: To evaluate the potential superiority of bailout angioplasty over standard treatment in cases of unsuccessful recanalisation (eTICI 0 to 2a) or residual severe stenosis (>70%) after thrombectomy in acute LVO patients within 24 hours of stroke onset.
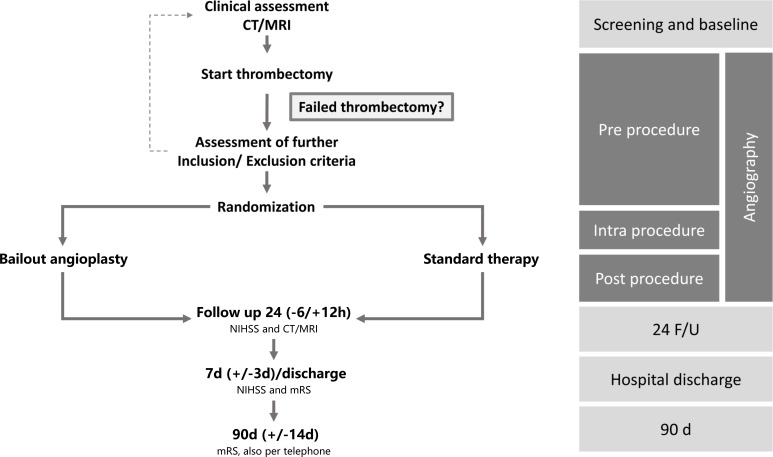
Design: This study is a multicentre, prospective, randomised, controlled clinical trial designed by investigators. It compares bailout angioplasty with standard therapy and follows an open-label treatment approach while maintaining a blinded outcome assessment (PROBE design). Our objective is to allocate 348 patients in a 1:1 ratio to either receive bailout angioplasty as an intervention or standard therapy as a control, following unsuccessful thrombectomy.
Outcome: The main measure of interest is the modified Rankin Scale (mRS) Score, which will be assessed in a blinded manner at 90 (±14) days following randomisation. The primary effect size will be determined using ordered logistic regression to calculate the common OR, representing the shift on the six-category mRS Scale at the 90-day mark. Additionally, the safety outcomes will be evaluated, including symptomatic intracranial haemorrhage within 18-36 hours, severe procedure-related complications and mortality within 90 (±14) days, among others.
Discussion: The ANGEL-REBOOT study aims to generate substantial evidence regarding the efficacy and safety of bailout intracranial angioplasty as a treatment option for patients with LVO who have experienced unsuccessful thrombectomy.
期刊介绍:
Stroke and Vascular Neurology (SVN) is the official journal of the Chinese Stroke Association. Supported by a team of renowned Editors, and fully Open Access, the journal encourages debate on controversial techniques, issues on health policy and social medicine.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


