Patrick L C Tapley, Martin Van der Vyver, Natalie G Coburn, Julie Hallet, Calvin Law, Rachel Roke, Paul J Karanicolas
{"title":"Rectus sheath catheters reduce opiate use in pancreaticoduodenectomy: a pre- and postintervention cohort study.","authors":"Patrick L C Tapley, Martin Van der Vyver, Natalie G Coburn, Julie Hallet, Calvin Law, Rachel Roke, Paul J Karanicolas","doi":"10.1503/cjs.006922","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Pancreaticoduodenectomy is the only curative option for patients with pancreatic cancer; however, pain remains a considerable problem postoperatively. With many centres moving away from using epidural analgesia, there is the need to evaluate alternative opiate sparing techniques for postoperative analgesia. We sought to determine if rectus sheath catheters (RSCs) had an opiate sparing and analgesic effect compared with standard care alone (opiate analgesia).</p><p><strong>Methods: </strong>We conducted a retrospective pre- and postintervention cohort study of patients undergoing pancreaticoduodenectomy at a single tertiary academic hospital in Toronto, Canada, between April 2018 and December 2019. All patients undergoing a pancreaticoduodenectomy were eligible for inclusion. Among the 101 patients identified, 84 (61 control, 23 RSCs) were analyzed after exclusion criteria were applied (epidural analgesia, admission to intensive care intubated or reintubated within the first 96 hours). The pre-intervention group received a semi-standardized course of analgesics, including intravenous hydromorphone, acetaminophen, ketamine, with or without nonsteroidal anti-inflammatory, and with or without intravenous lidocaine; the latter 2 drugs were at the individual anesthesiologist and surgeon's preference. For the postintervention group, the same course of analgesics were used, with the addition of RSCs. These were inserted at the end of the operation, with a loading dose of ropivacaine administered and followed by a programmed intermittent bolus regime for 72-96 hours. The primary outcome measure was total postoperative opiate consumption (oral morphine equivalents). Secondary outcomes included pain scores (numeric rating scale) and treatment-related adverse effects.</p><p><strong>Results: </strong>Opiate consumption (oral morphine equivalents) at 96 hours was significantly lower (median 188 mg, interquartile range [IQR] 112-228 v. 242.4 mg, IQR 166.8-352) with and without RSC, respectively (<i>p</i> = 0.01). The RSC group used significantly less opiates at each time point from 24 hours postoperatively, with no significant difference in pain scores between the groups and no significant catheter-related complications.</p><p><strong>Conclusion: </strong>The use of RSCs was associated with significant reductions in postoperative opiate consumption. Given the ease of placement and management, with minimal complications, RSCs should be incorporated into a course of postoperative multimodal analgesia. A large scale randomized controlled trial should be conducted to further investigate these findings.</p>","PeriodicalId":9573,"journal":{"name":"Canadian Journal of Surgery","volume":"66 4","pages":"E367-E377"},"PeriodicalIF":2.2000,"publicationDate":"2023-07-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a9/9f/066E367.PMC10355997.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1503/cjs.006922","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/7/1 0:00:00","PubModel":"Print","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Pancreaticoduodenectomy is the only curative option for patients with pancreatic cancer; however, pain remains a considerable problem postoperatively. With many centres moving away from using epidural analgesia, there is the need to evaluate alternative opiate sparing techniques for postoperative analgesia. We sought to determine if rectus sheath catheters (RSCs) had an opiate sparing and analgesic effect compared with standard care alone (opiate analgesia).
Methods: We conducted a retrospective pre- and postintervention cohort study of patients undergoing pancreaticoduodenectomy at a single tertiary academic hospital in Toronto, Canada, between April 2018 and December 2019. All patients undergoing a pancreaticoduodenectomy were eligible for inclusion. Among the 101 patients identified, 84 (61 control, 23 RSCs) were analyzed after exclusion criteria were applied (epidural analgesia, admission to intensive care intubated or reintubated within the first 96 hours). The pre-intervention group received a semi-standardized course of analgesics, including intravenous hydromorphone, acetaminophen, ketamine, with or without nonsteroidal anti-inflammatory, and with or without intravenous lidocaine; the latter 2 drugs were at the individual anesthesiologist and surgeon's preference. For the postintervention group, the same course of analgesics were used, with the addition of RSCs. These were inserted at the end of the operation, with a loading dose of ropivacaine administered and followed by a programmed intermittent bolus regime for 72-96 hours. The primary outcome measure was total postoperative opiate consumption (oral morphine equivalents). Secondary outcomes included pain scores (numeric rating scale) and treatment-related adverse effects.
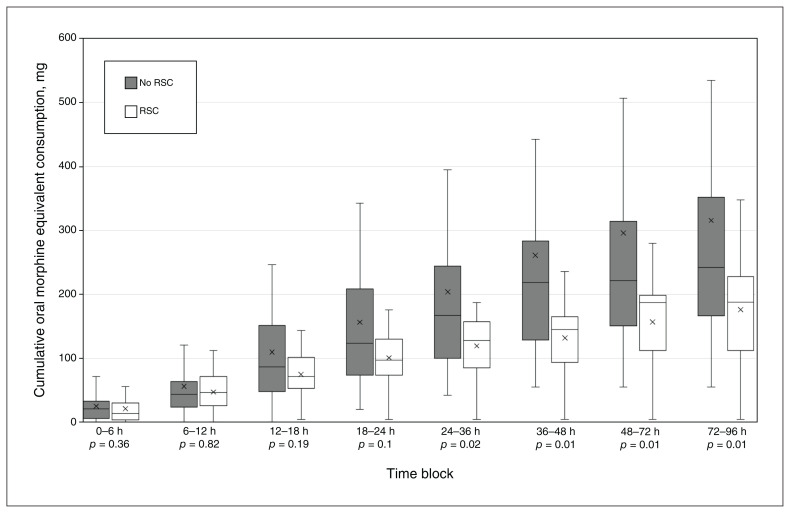
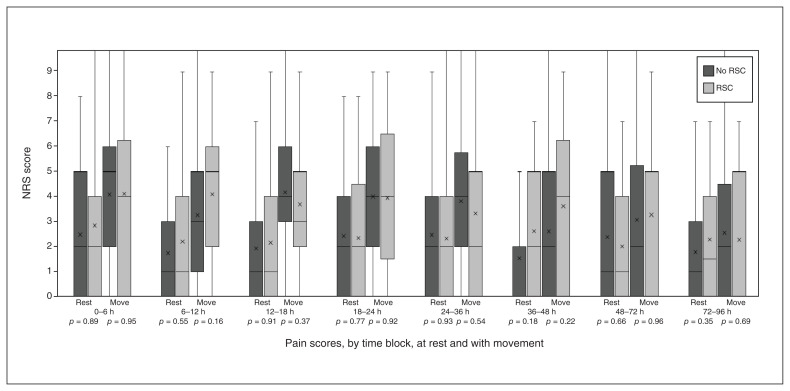
Results: Opiate consumption (oral morphine equivalents) at 96 hours was significantly lower (median 188 mg, interquartile range [IQR] 112-228 v. 242.4 mg, IQR 166.8-352) with and without RSC, respectively (p = 0.01). The RSC group used significantly less opiates at each time point from 24 hours postoperatively, with no significant difference in pain scores between the groups and no significant catheter-related complications.
Conclusion: The use of RSCs was associated with significant reductions in postoperative opiate consumption. Given the ease of placement and management, with minimal complications, RSCs should be incorporated into a course of postoperative multimodal analgesia. A large scale randomized controlled trial should be conducted to further investigate these findings.
期刊介绍:
The mission of CJS is to contribute to the meaningful continuing medical education of Canadian surgical specialists, and to provide surgeons with an effective vehicle for the dissemination of observations in the areas of clinical and basic science research.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


