{"title":"Acute Exacerbation of COPD.","authors":"Dominic Pappas, Amrita Vempati","doi":"10.21980/J8V070","DOIUrl":null,"url":null,"abstract":"<p><strong>Audience: </strong>This case is targeted to emergency medicine residents of all levels.</p><p><strong>Introduction: </strong>Shortness of breath (SOB) is one of the top ten most common chief complaints seen in the Emergency Department, accounting for close to 10% of presenting complaints.1 An acute exacerbation of chronic obstructive pulmonary disease (AECOPD) is a frequent culprit, accounting for roughly 15.4 million visits and 730,000 hospitalizations per year.2 The diagnosis of treatment of mild to moderate AECOPD can be relatively uncomplicated; however, multiple factors can increase the complexity of management and pose additional challenges that the emergency physician (EP) must be prepared for. Severe AECOPD can necessitate the need for both Non-invasive positive pressure ventilator (NIPPV) such as bi-level positive airway pressure (BiPAP) as well as emergent intubation. Furthermore, managing the ventilator settings in patients with an AECOPD is far from routine, requiring an intricate understanding of pulmonary physiology.3.</p><p><strong>Educational objectives: </strong>By the end of this simulation, learners will be able to (1) assess for causes of severe shortness of breath, (2) manage severe COPD exacerbation by administering appropriate medications, (3) identify worsening clinical status and initiate NIPPV, (4) assess the causes of hypoxia after establishing endotracheal intubation and, (5) identify indication for needle decompression and perform chest tube thoracostomy.</p><p><strong>Educational methods: </strong>This simulation was conducted with a high-fidelity mannequin with a separate low fidelity chest tube mannequin that allowed for hands-on practice placing a chest tube. A total of 16 PGY-1 residents participated in the simulated patient encounter.</p><p><strong>Research methods: </strong>Following the simulation and debrief session, all residents were sent a Likert scale survey via surveymonkey.com to assess the educational quality of the simulation. The survey contained the following questions; 1) Overall, this simulation was realistic and could represent a patient presentation in the Emergency Department, 2) Overall, the case contained complexity that challenged me as a learner, 3) This case helped to expand my medical knowledge, 4) I feel more confident in diagnosing and treating AECOPD, 5) I feel more confident in recognizing the indications for NIPPV and intubation, 6) This simulation offered an opportunity to improve my procedural skills, 7) I feel more confident in setting up the ventilator, 8) I feel more confident in addressing ventilator alarms.</p><p><strong>Results: </strong>Following the simulation and debrief session, all the participants (n=16), were provided a survey to assess the educational quality of the simulation. There were a total of 12 respondents and a hundred percent of them agreed or strongly agreed that the case contained complexity that challenged them. All of the respondents agreed that the simulation case was realistic and that the case helped expand their medical knowledge. Furthermore, all the learners agreed or strongly agreed that the case helped them in improving their procedural skills.</p><p><strong>Discussion: </strong>This case combines a mixture of high fidelity and medium fidelity components to encompass both clinical knowledge and procedural skills. This case is effective in expanding beyond the basic approach to managing an AECOPD patient and forces learners to address clinical deterioration, escalate airway interventions, manage ventilator settings, and address ventilator alarms, including placement of a chest tube. Residents commented that this case was very realistic and particularly challenging because it highlighted gaps in their clinical knowledge and procedural skills. Residents were most challenged by identifying when to escalate care as well as how to manage ventilator settings in AECOPD patients.</p><p><strong>Topics: </strong>Acute exacerbation COPD, intubation, positive pressure ventilation, ventilator alarms, chest tube thoracostomy.</p>","PeriodicalId":73721,"journal":{"name":"Journal of education & teaching in emergency medicine","volume":"8 2","pages":"S35-S61"},"PeriodicalIF":0.0000,"publicationDate":"2023-04-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10332676/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of education & teaching in emergency medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21980/J8V070","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/4/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Audience: This case is targeted to emergency medicine residents of all levels.
Introduction: Shortness of breath (SOB) is one of the top ten most common chief complaints seen in the Emergency Department, accounting for close to 10% of presenting complaints.1 An acute exacerbation of chronic obstructive pulmonary disease (AECOPD) is a frequent culprit, accounting for roughly 15.4 million visits and 730,000 hospitalizations per year.2 The diagnosis of treatment of mild to moderate AECOPD can be relatively uncomplicated; however, multiple factors can increase the complexity of management and pose additional challenges that the emergency physician (EP) must be prepared for. Severe AECOPD can necessitate the need for both Non-invasive positive pressure ventilator (NIPPV) such as bi-level positive airway pressure (BiPAP) as well as emergent intubation. Furthermore, managing the ventilator settings in patients with an AECOPD is far from routine, requiring an intricate understanding of pulmonary physiology.3.
Educational objectives: By the end of this simulation, learners will be able to (1) assess for causes of severe shortness of breath, (2) manage severe COPD exacerbation by administering appropriate medications, (3) identify worsening clinical status and initiate NIPPV, (4) assess the causes of hypoxia after establishing endotracheal intubation and, (5) identify indication for needle decompression and perform chest tube thoracostomy.
Educational methods: This simulation was conducted with a high-fidelity mannequin with a separate low fidelity chest tube mannequin that allowed for hands-on practice placing a chest tube. A total of 16 PGY-1 residents participated in the simulated patient encounter.
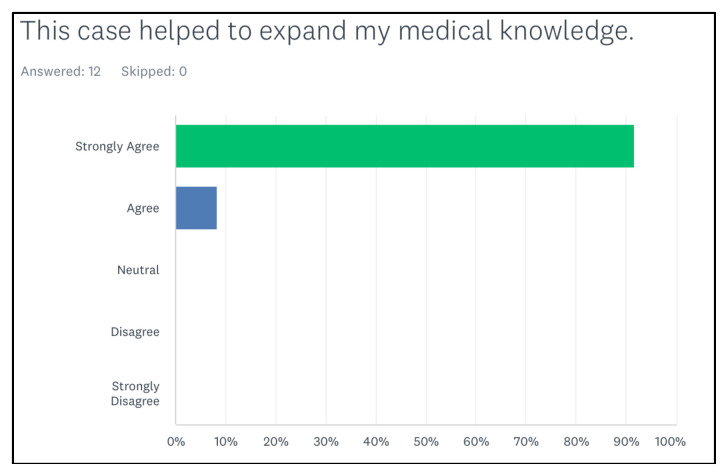
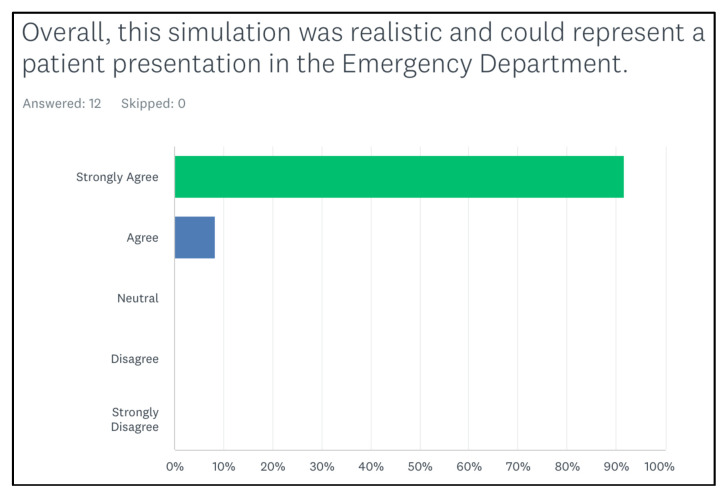
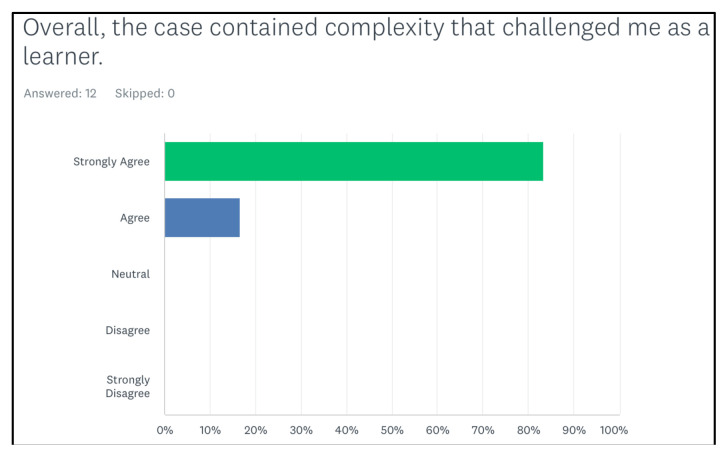
Research methods: Following the simulation and debrief session, all residents were sent a Likert scale survey via surveymonkey.com to assess the educational quality of the simulation. The survey contained the following questions; 1) Overall, this simulation was realistic and could represent a patient presentation in the Emergency Department, 2) Overall, the case contained complexity that challenged me as a learner, 3) This case helped to expand my medical knowledge, 4) I feel more confident in diagnosing and treating AECOPD, 5) I feel more confident in recognizing the indications for NIPPV and intubation, 6) This simulation offered an opportunity to improve my procedural skills, 7) I feel more confident in setting up the ventilator, 8) I feel more confident in addressing ventilator alarms.
Results: Following the simulation and debrief session, all the participants (n=16), were provided a survey to assess the educational quality of the simulation. There were a total of 12 respondents and a hundred percent of them agreed or strongly agreed that the case contained complexity that challenged them. All of the respondents agreed that the simulation case was realistic and that the case helped expand their medical knowledge. Furthermore, all the learners agreed or strongly agreed that the case helped them in improving their procedural skills.
Discussion: This case combines a mixture of high fidelity and medium fidelity components to encompass both clinical knowledge and procedural skills. This case is effective in expanding beyond the basic approach to managing an AECOPD patient and forces learners to address clinical deterioration, escalate airway interventions, manage ventilator settings, and address ventilator alarms, including placement of a chest tube. Residents commented that this case was very realistic and particularly challenging because it highlighted gaps in their clinical knowledge and procedural skills. Residents were most challenged by identifying when to escalate care as well as how to manage ventilator settings in AECOPD patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


