Nicole H Goldhaber, Robin L Schaefer, Roman Martinez, Andrew Graham, Elizabeth Malachowski, Lisa P Rhodes, Ruth S Waterman, Kristin L Mekeel, Brian J Clay, Michael McHale
{"title":"Surgical pit crew: initiative to optimise measurement and accountability for operating room turnover time.","authors":"Nicole H Goldhaber, Robin L Schaefer, Roman Martinez, Andrew Graham, Elizabeth Malachowski, Lisa P Rhodes, Ruth S Waterman, Kristin L Mekeel, Brian J Clay, Michael McHale","doi":"10.1136/bmjhci-2023-100741","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objectives: </strong>Turnover time (TOT), defined as the time between surgical cases in the same operating room (OR), is often perceived to be lengthy without clear cause. With the aim of optimising and standardising OR turnover processes and decreasing TOT, we developed an innovative and staff-interactive TOT measurement method.</p><p><strong>Methods: </strong>We divided TOT into task-based segments and created buttons on the electronic health record (EHR) default prelogin screen for appropriate staff workflows to collect more granular data. We created submeasures, including 'clean-up start', 'clean-up complete', 'set-up start' and 'room ready for patient', to calculate environmental services (EVS) response time, EVS cleaning time, room set-up response time, room set-up time and time to room accordingly.</p><p><strong>Results: </strong>Since developing and implementing these workflows, measures have demonstrated excellent staff adoption. Median times of EVS response and cleaning have decreased significantly at our main hospital ORs and ambulatory surgery centre.</p><p><strong>Conclusion: </strong>OR delays are costly to hospital systems. TOT, in particular, has been recognised as a potential dissatisfier and cause of delay in the perioperative environment. Viewing TOT as one finite entity and not a series of necessary tasks by a variety of team members limits the possibility of critical assessment and improvement. By dividing the measurement of TOT into respective segments necessary to transition the room at the completion of one case to the onset of another, valuable insight was gained into the causes associated with turnover delays, which increased awareness and improved accountability of staff members to complete assigned tasks efficiently.</p>","PeriodicalId":9050,"journal":{"name":"BMJ Health & Care Informatics","volume":"30 1","pages":""},"PeriodicalIF":4.1000,"publicationDate":"2023-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a1/22/bmjhci-2023-100741.PMC10351225.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Health & Care Informatics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjhci-2023-100741","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Background and objectives: Turnover time (TOT), defined as the time between surgical cases in the same operating room (OR), is often perceived to be lengthy without clear cause. With the aim of optimising and standardising OR turnover processes and decreasing TOT, we developed an innovative and staff-interactive TOT measurement method.
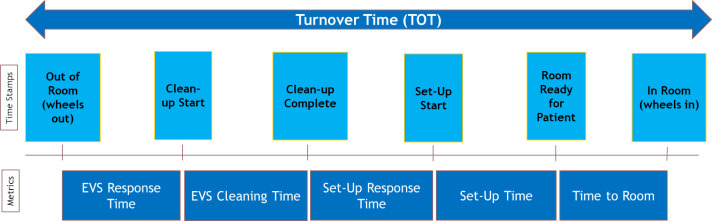
Methods: We divided TOT into task-based segments and created buttons on the electronic health record (EHR) default prelogin screen for appropriate staff workflows to collect more granular data. We created submeasures, including 'clean-up start', 'clean-up complete', 'set-up start' and 'room ready for patient', to calculate environmental services (EVS) response time, EVS cleaning time, room set-up response time, room set-up time and time to room accordingly.
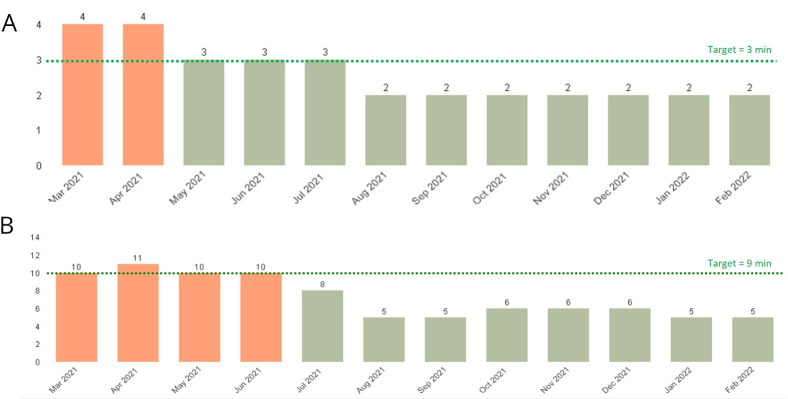
Results: Since developing and implementing these workflows, measures have demonstrated excellent staff adoption. Median times of EVS response and cleaning have decreased significantly at our main hospital ORs and ambulatory surgery centre.
Conclusion: OR delays are costly to hospital systems. TOT, in particular, has been recognised as a potential dissatisfier and cause of delay in the perioperative environment. Viewing TOT as one finite entity and not a series of necessary tasks by a variety of team members limits the possibility of critical assessment and improvement. By dividing the measurement of TOT into respective segments necessary to transition the room at the completion of one case to the onset of another, valuable insight was gained into the causes associated with turnover delays, which increased awareness and improved accountability of staff members to complete assigned tasks efficiently.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


