William Mitchell, Thomas Roser, Jessica Heard, Shankar Logarajah, John Ok, John Jay, Houssam Osman, D Rohan Jeyarajah
{"title":"Regional Anesthetic Use in Trans-Hiatal Esophagectomy. Are They Worth Consideration? A Case Series.","authors":"William Mitchell, Thomas Roser, Jessica Heard, Shankar Logarajah, John Ok, John Jay, Houssam Osman, D Rohan Jeyarajah","doi":"10.2147/LRA.S398331","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Esophagectomy traditionally has high levels of perioperative morbidity and mortality due to surgical techniques and case complexity. While thoracic epidural analgesia (TEA) is considered first-line for postoperative analgesia after esophagectomy, complications can arise related to its sympathectomy and mobility impairment. Additionally, it has been shown that postoperative outcomes are improved with early extubation following esophagectomy. Our aim is to describe the impact of transversus abdominis plane (TAP) blocks on extubation rates following esophagectomy when uncoupled from TEA.</p><p><strong>Methods: </strong>This is a case series of 42 patients who underwent trans-hiatal esophagectomy between 2019 and 2022 who received a TAP block without TEA. The primary outcomes of interest were the rates of extubation within the operating room (OR) and reintubation. Secondary outcomes included: intensive care unit (ICU) and hospital length of stay (LOS), opioid pain medication use, post-operative hypotension, fluid administration, postoperative pain scores, development of anastomotic leak, and 30-day readmission.</p><p><strong>Results: </strong>The mean age at operation was 63 years and 97.6% of patients were represented by American Society of Anesthesia (ASA) physical status class III or IV. Thirty-four (81%) patients immediately extubated postoperatively. Nine patients (21.4%) underwent reintubation during their hospital course. Only seven patients (16.7%) required vasopressors postoperatively. The median LOS was five days in the ICU and 10 days in the hospital. TAP block alone was found to be equivalent to TAP with additional regional blocks (TAP+) on the basis of immediate extubation, reintubation, ICU and hospital LOS, and reported postoperative pain.</p><p><strong>Conclusion: </strong>The results of this study demonstrated immediate extubation is possible using TAP blocks while limiting post-operative hypotension and fluid administration. This was shown despite the elevated comorbidity burden of this study's population. Overall, this study supports the use of TAP blocks as a possible alternative for primary analgesia in patients undergoing trans-hiatal esophagectomy.</p><p><strong>Trial registration: </strong>This study includes participants who were retrospectively registered. IRB# 037.HPB.2018.R.</p>","PeriodicalId":18203,"journal":{"name":"Local and Regional Anesthesia","volume":"16 ","pages":"99-111"},"PeriodicalIF":1.9000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/13/5c/lra-16-99.PMC10349603.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Local and Regional Anesthesia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/LRA.S398331","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Esophagectomy traditionally has high levels of perioperative morbidity and mortality due to surgical techniques and case complexity. While thoracic epidural analgesia (TEA) is considered first-line for postoperative analgesia after esophagectomy, complications can arise related to its sympathectomy and mobility impairment. Additionally, it has been shown that postoperative outcomes are improved with early extubation following esophagectomy. Our aim is to describe the impact of transversus abdominis plane (TAP) blocks on extubation rates following esophagectomy when uncoupled from TEA.
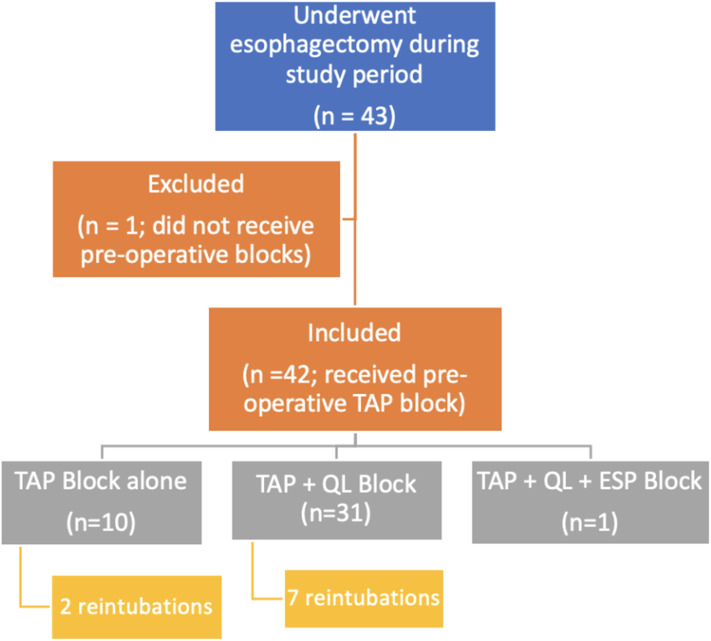
Methods: This is a case series of 42 patients who underwent trans-hiatal esophagectomy between 2019 and 2022 who received a TAP block without TEA. The primary outcomes of interest were the rates of extubation within the operating room (OR) and reintubation. Secondary outcomes included: intensive care unit (ICU) and hospital length of stay (LOS), opioid pain medication use, post-operative hypotension, fluid administration, postoperative pain scores, development of anastomotic leak, and 30-day readmission.
Results: The mean age at operation was 63 years and 97.6% of patients were represented by American Society of Anesthesia (ASA) physical status class III or IV. Thirty-four (81%) patients immediately extubated postoperatively. Nine patients (21.4%) underwent reintubation during their hospital course. Only seven patients (16.7%) required vasopressors postoperatively. The median LOS was five days in the ICU and 10 days in the hospital. TAP block alone was found to be equivalent to TAP with additional regional blocks (TAP+) on the basis of immediate extubation, reintubation, ICU and hospital LOS, and reported postoperative pain.
Conclusion: The results of this study demonstrated immediate extubation is possible using TAP blocks while limiting post-operative hypotension and fluid administration. This was shown despite the elevated comorbidity burden of this study's population. Overall, this study supports the use of TAP blocks as a possible alternative for primary analgesia in patients undergoing trans-hiatal esophagectomy.
Trial registration: This study includes participants who were retrospectively registered. IRB# 037.HPB.2018.R.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


